As a veterinary dentist, much of what I do revolves around the discipline of oral surgical oncology. An average appointment day typically involves seeing at least a few dogs or cats with oral masses. In cats, those masses are frequently diagnosed as squamous cell carcinoma. In dogs, benign tumors are more common, with peripheral odontogenic fibromas (POFs) leading the way.
A look at POFs
Peripheral odontogenic fibromas, previously referred to as fibromatous and ossifying epulis, can manifest in a variety of shapes, but they all arise from the attached gingiva or gingival margin, usually in an area where a tooth is present.
Radiographically, POFs cause minimal to no bony lysis. Mineralization may be seen radiographically in the center of the mass. This finding can be a helpful diagnostic tool since it is rare for other gingival tumors to arise from the gingiva or have a mineralized center, while not causing bony lysis.
Some POFs will not show evidence of a mineralized center: these are the fibromatous instead of the ossifying variant. POFs can adversely affect adjacent teeth, but since they are typically slowly growing, they rarely result in tooth resorption. Instead, POFs often act like orthodontic devices, moving apart the teeth as the tumor grows between them.
POFs are odontogenic tumors, which means they arise from cells responsible for forming teeth. Cells within the periodontal ligament or within the gingival connective tissue that are remnants of tooth development can overgrow their normal boundaries and manifest as either a pedunculated or broad-based firm, pink mass. These masses are typically non-ulcerated, but as they enlarge, they can become ulcerated caused by trauma from opposing teeth.
Presentation
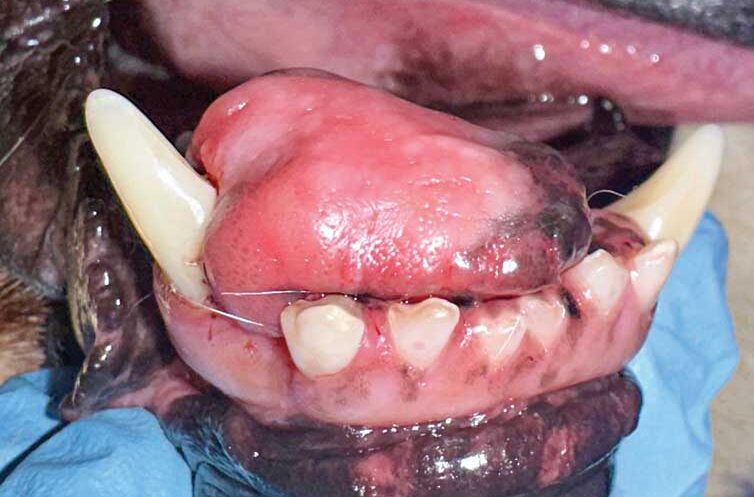
We recently saw a patient that was a good reminder POFs can sometimes be quite large. Isaac, an eight-year-old male neutered retriever/husky mix, was presented for evaluation of a 3 cm x 3 cm x 2 cm mass arising from the lingual surface of teeth 403 and 404. The mass was first noted five months earlier, and at that time, it was considered to be approximately 1 cm in diameter on awake examination.
Even though the mass was reported to be approximately 1 cm in diameter at the time it was first noted, the owner did not feel the size of the mass had changed significantly since first noted. Recently, Isaac began to drink water more sloppily and took longer to eat his meals.
Diagnosis
Blood work was nonremarkable except for a mildly elevated globulin level at 3.7 g/dL (reference range 1.6-3.6 g/dL). Isaac was placed under anesthesia. Anesthetized oral examination was within normal limits except for a firm mass measuring approximately 3 cm x 3 cm x 2 cm, arising from the lingual surface of the gingiva of teeth 403 and 404 (Figure 1).
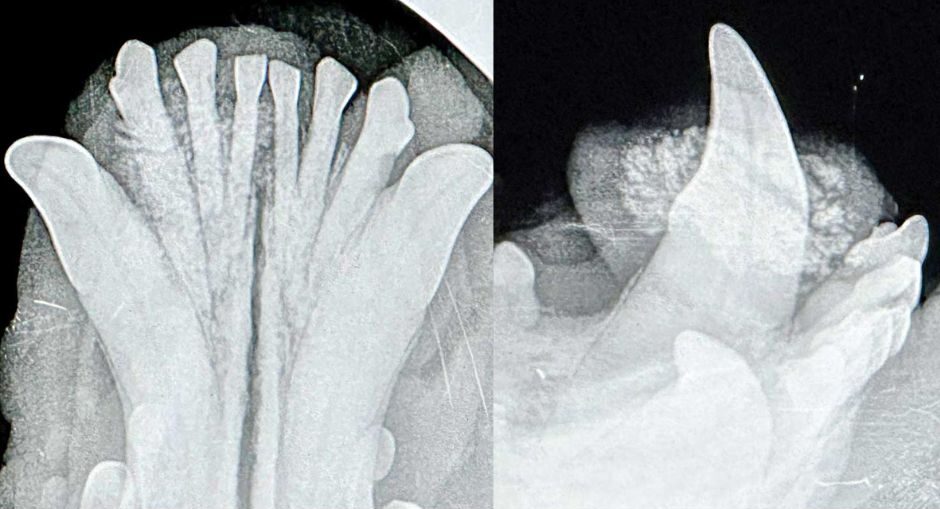
Dental radiographs were obtained. The occlusal view of the rostral mandible showed some evidence of mineralization in the absence of any significant bony lysis (Figure 2 A). This view and the anesthetized examination also showed there was increased space between teeth 403 and 404 compared to the interdental space between 303 and 304. This was likely due to the slow growth of the tumor resulting in movement of the smaller of the two teeth as the tumor enlarged.
A lateral view of the rostral mandible with a size 4 phosphor plate was able to capture the impressive amount of mineralization within the mass (Figure 2 B).
Biopsy
When performing a biopsy on a mineralized mass, a scalpel blade or a biopsy punch will not cut it (pun intended). For incisional biopsy of such a mass, use a diamond bur on a water-cooled high-speed handpiece or a rongeur to obtain a sample. In Isaac’s case, the clinical (and especially radiographic) appearance led us to believe we were dealing with a peripheral odontogenic fibroma, so we opted to forego the incisional biopsy and move forward with a curative intent surgery.
An en bloc piece that included the mass, attached gingiva of 403 and 404, the teeth, and coronal portion of the roots, were submitted in a single piece. The roots of 403 and 404 were removed, the alveoli were curetted, and a diamond bur was used to remove additional bone and smooth down rough edges. The site was then closed with a mucoperiosteal flap of labial mucosa. Histopathology confirmed the diagnosis of peripheral odontogenic fibroma. Isaac did well in the postoperative period.
This case is a good reminder not all large masses are malignant. Clinical and radiographic information obtained intraoperatively can help in decision making of whether to pursue an incisional vs. excisional biopsy.
John R. Lewis, VMD, DAVDC Fellow, AVDC OMFS, practices at Veterinary Dentistry Specialists and teaches at Silo Academy Education Center, both in Chadds Ford, Pa.