
I recently saw a case that was a good reminder of the varying appearances of squamous cell carcinoma (SCC). Leo, a four-year-old male miniature schnauzer, was presented to me to repair a puncture wound in his soft palate. Over the prior five months, Leo had not been his playful self. He showed signs of oral discomfort.
Sedated oral examination at Leo’s primary care vet revealed what appeared to be a puncture wound on the left caudal soft palate. Leo was also diagnosed with Lyme disease and was treated with doxycycline and carprofen. Leo showed improvement when on carprofen, but once the medication was discontinued, he again was in pain. Antibiotics did not seem to resolve the clinical signs.
Photos courtesy John R. Lewis
Presentation
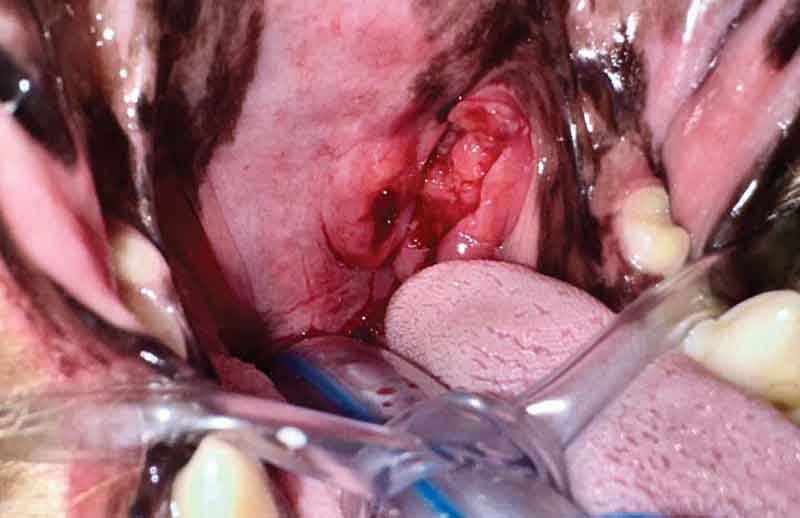
When I saw Leo for consultation, his owner reported his appetite was diminished. On physical examination, he cried in pain when I opened his mouth fully. During that brief glimpse, I saw the defect in the soft palate that was described to me by the owner and Leo’s referring veterinarian. The defect looked like the photos taken during a recent sedated exam. It was approximately 7 mm long and 3 mm wide and was located in the caudal soft palate, situated between the midline of the soft palate and the left tonsil (Figure 1).
Leo’s owners were interested in repair of the palatal defect and exploration for any foreign material that was preventing healing. They recalled an incident prior to the onset of clinical signs where Leo was caught chewing on a piece of plastic that made them wonder if a piece of foreign material was preventing healing.
We anesthetized Leo. Cone-beam CT scan of the head showed the defect in the palate did not extend full-thickness into the nasopharynx. The left caudal soft palate showed diffuse thickening in the dorsoventral dimension, and the left tympanic bulla was filled with a soft tissue density.
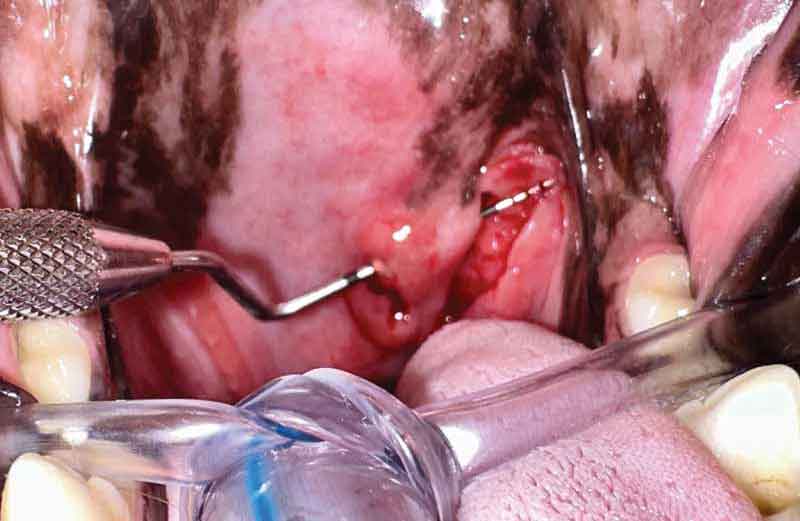
Probing of the palatal defect confirmed it was not full-thickness, but instead communicated with the left tonsil (Figure 2). The tract between the defect and the tonsil was explored, and revealed a lobulated, red, friable soft tissue similar to the tissue seen in the left tonsillar crypt. The areas directly rostral and caudal to the palatal defect palpated as thickened and more firm than normal. The mandibular lymph nodes palpated within normal limits on both the right and left sides.
The palatal defect and tonsillar crypt areas were explored. No foreign material was found. The lobulated tissue was biopsied and the tract between the palatal defect and the tonsil was cultured. The defect in the palate was closed with 5-0 poliglecaprone 25 in a simple continuous pattern.
Leo was discharged the same day, and we showed the CT scan to his owners and discussed possible diagnoses. Squamous cell carcinoma was discussed as a possibility, but we hoped that at Leo’s young age we were dealing with something else that was mimicking SCC. It was discussed that unfortunately, if the diagnosis of SCC was made, the diffuse nature of the palatal and tonsil changes would prevent us from offering a curative intent surgery.
Assessment
The CT scan was sent to a radiologist who reported: “The left tympanic bulla is filled with homogeneous soft tissue attenuating material. Its bony margins are similar in thickness to the contralateral one and considered normal. The external ear canal on the left side is within normal limits. An asymmetric swelling of the soft palate is visible and characterized by mild obliteration of the left ventral aspect of the nasopharynx, as well as bulging into the oral cavity. A well-defined gas attenuating accumulation is present within the swollen soft tissues. Assessment: left-sided cavitary (soft tissue with gas) mass of the soft palate with mild obliteration of the nasopharynx.
Given the gas inclusion, the mass is consistent with an abscess. No radiopaque foreign body could be identified. A radiotransparent foreign body cannot be ruled out. The mass could also be the result from a puncture wound from a foreign body that is no longer present. A neoplasia cannot be ruled out but seems less likely.”
The gas-attenuating accumulation described by the radiologist equated to the visible defect in the palate that communicated with the tonsil but not with the nasopharynx (Figure 3). One possible explanation for the soft tissue density within the left tympanic bulla may be related to an obscure detail of anatomy in the area: the Eustachian tube. The Eustachian tube travels from the middle ear to the lateral wall of the nasopharynx. The tube functions to aerate the middle ear and clear the middle ear of material. The tube is a physiologic valve, and when the valve fails to function properly, the middle ear may be affected by otitis media and/or abnormal accumulation of fluid.
It may be the swelling/mass in the palate/tonsil area resulted in blockage of the Eustachian tube, preventing normal drainage of the middle ear. Another possible reason for soft tissue density within the tympanic bulla would be if the tonsillar SCC was able to migrate dorsally through the Eustachian tube into the middle ear.
Diagnosis
Histopathology results were received one week later. It revealed the diagnosis none of us wanted to hear: tonsillar squamous cell carcinoma. Having to tell owners, such as Leo’s parents, their pet has cancer is always difficult. It is especially difficult when it is a young dog that has an inoperable cancer.
Though shocked and distraught by the unfortunate news their four-year-old schnauzer has cancer, Leo’s owners wasted no time in pursuing treatment options. Leo has already visited a medical oncologist and may begin radiation treatment soon. Fingers crossed for this wonderful dog!

John R. Lewis, VMD, DAVDC, FF-OMFS practices and teaches at Veterinary Dentistry Specialists and Silo Academy Education Center, both located in Chadds Ford, Pa.
Reference
- Mas A, Blackwood L, Cripps P, Murphy S, De Vos J, Dervisis N, Martano M, Polton GA. Canine tonsillar squamous cell carcinoma — a multi-centre retrospective review of 44 clinical cases. J Small Anim Pract. 2011;52(7):359-364. https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1748-5827.2011.01075.x