In last month’s column, we discussed a double flap technique for persistent oronasal fistulas. This month, we will continue the discussion in the context of larger acquired oronasal defects.
Case in point
Ace, a middle-aged male neutered black Labrador, was presented for treatment of a left maxillary mass. The mass was originally suspected to be a tooth root abscess associated with the left maxillary fourth premolar (tooth 208), but when the swelling persisted after extraction (Figure 1), Ace had a biopsy performed by a veterinary dentist.

Results revealed the dreaded diagnosis of oral fibrosarcoma, which is a difficult cancer to obtain clean margins on due to microscopic tendrils of neoplastic tissue that quietly extend into the apparently normal surrounding soft tissue. Ace was referred to me for curative intent surgery.
After discussing options with Ace’s owners, it was decided that we would attempt a left maxillectomy, ventral orbitectomy, and rostral zygomectomy in addition to removing a large area of skin over the palpable tumor (Figure 2). A rotation skin flap would be raised, using the skin caudal to the excised area, to close the cutaneous defect (Figure 3), and a thin piece of remaining lip mucosa was used to close the intraoral defect.


Running into complications
Unfortunately, approximately one week after his maxillectomy, Ace started to show signs of possible intraoral dehiscence: nasal discharge and sneezing associated with eating and drinking. An awake reexamination showed a large palatal defect (approximately 9 cm x 5 cm, Figure 4).
Rather than rushing in to repair the defect immediately, we prescribed antibiotics for Ace to minimize the chances of aspiration pneumonia and to allow the tissues to epithelialize fully prior to pursuing repair of the defect. Eight weeks later, we placed Ace under anesthesia to attempt to repair the defect (Figure 5).


Fixing the problem
After eight weeks, repair of the defect was attempted with a double flap
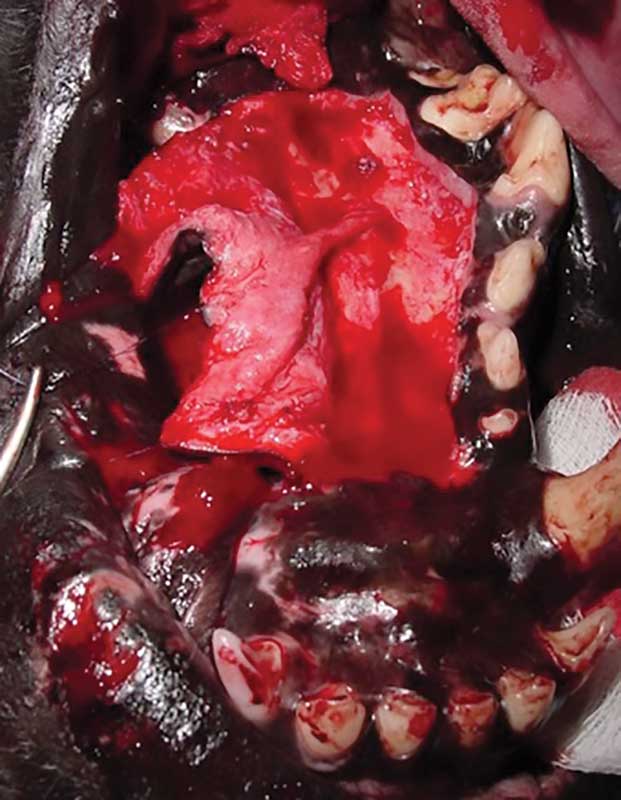
technique. The first flap was raised using the soft tissue over the hard palate medial to the defect. The flap was connected by a hinge and retained blood supply from the right major palatine artery (Figure 6). The distal edge of this flap was sutured to an incision made lateral to the defect to raise a second flap of remaining labial/buccal mucosa.
Since so much labial/buccal mucosa was removed during the first surgery, flap two was unable to fully cover the donor site of flap one (Figure 7). A portion of the donor site of flap one was left exposed to granulate in via second-intention healing.

The difference
What is the difference between an oronasal defect and an oroantral defect? An oronasal defect communicates with the nasal passage, whereas are oroantral fistula occurs more caudally and communicates with the maxillary recess. In this case, the defect was large enough to communicate with both the nasal passage and the left maxillary recess.
Post-op and recovery
Ace did well in the postoperative period, and approximately four weeks after the revision surgery, the Labrador was sedated to assess healing. No communications with the nasal passage or maxillary recess were seen. The donor site of flap one was covered with healthy granulation tissue and was already partially epithelialized (Figure 8). No evidence of recurrence of the fibrosarcoma was noted, which was consistent the clean margins noted by the pathologist.

This case is a good example that even large defects of the hard palate can be surgically repaired. Double flaps are particularly helpful to provide support to oral epithelium to minimize tension on the more superficial flap. Even specialists see dehiscence occur with some of their cases.
The key is to develop a revision plan that is based on good surgical principles and addresses shortcomings of the original closure. In Ace’s case, we applied a tape muzzle after the second surgery. This limited the ability to open the mouth and decreased tension on the suture line.
John R. Lewis, VMD, DAVDC, Fellow AVDC OMFS, practices at Veterinary Dentistry Specialists and teaches at Silo Academy Education Center, both in Chadds Ford, Pa.