Unfortunately, despite our best effort to prevent postoperative complications, it is impossible to eliminate them completely. It is important to accurately log and review postoperative complications and some form of surgical auditing should be in place at all surgical facilities.
As the saying goes, “Hope for the best but prepare for the worst.” Dealing with complications starts with preparing for them. The first stage of preparation should be to warn the client of some of the commonly encountered surgical complications.
When talking with clients, it can help to break down complications into those that may occur intraoperatively, what may occur immediately postoperatively, and any potential longer-term complications. While it is hard to predict what may or may not go wrong, it is useful to emphasize to clients that surgical complications may result in the need for more surgery, prolonged hospitalization, or frequent hospital visits. It is also prudent to mention there is usually a cost associated with treating a surgical complication.
If a complication does occur during surgery, there are a few important steps to take. If something is bleeding, the first thing to do is apply pressure to control it. Take a deep breath and tell everyone you are working with what is happening. Plan a strategy to deal with it and include systemic treatment, such as starting a fluid bolus.
Try to think about what equipment you may need, such as suture material, abdominal retractors etc., and ask someone to scrub in and assist you because an extra pair of hands can really help when things are not going as planned. Have someone note the time and ask them to give you a notice every two minutes (or whatever time interval seems appropriate). It is amazing how our perception of time changes when we are very stressed and sometimes it can feel like you have been trying to find the bleeding ovarian stump for ages, when it has only been 60 seconds, so knowing exactly how much time has passed can really help.
Once the complication has been dealt with, take a second to reset and refocus as it is easy at this point to lose concentration and do something you would not normally do, such as forget to count sponges. Short-term postoperative complications are most frequently superficial surgical site infections, seromas, and suture reactions.
Superficial surgical site infection
Topical treatment for superficial surgical site infections allows high concentrations of antibacterial substances to be delivered to the site of infection. Silver wound dressings and antibacterial hypochlorous acid wound sprays are some of the most frequently utilized topical products in our clinic.
Antibiotics should be targeted at the most likely bacterial species based on the location of the surgical site and then adjusted based on culture and sensitivity results. Culture results are most accurate following an initial cleaning of the site to reduce contamination and if a small piece of tissue from the affected area is submitted rather than a swab of fluid.1
Seromas
Seromas usually develop due to excessive dead space, extensive surgical trauma, or sometimes due to over activity of the patient. Seromas can be differentiated from an abscess by the lack of pain, lack of heat, and through cytological evaluation. If cytology is performed, it is important a strict aseptic technique is used, and the tract is immediately covered with a sterile dressing. Iatrogenic infection following fine needle aspirate (FNA) and/or drainage is possible and, therefore, cytology may not always be required for a presumptive diagnosis.
Ultrasound can be used as a non-invasive diagnostic tool. Most seromas will be in the subcutaneous space and have clear, black fluid on ultrasonography compared to the often-hyperechoic fluid of an abscess.
An uncomplicated seroma should not impede wound healing and can be treated with intermittent warm packing, a reduction of the patient’s activity, and the tincture of time. Sometimes the application of a bandage can help apply some pressure and encourage redistribution of fluid. Rarely, a very large seroma will require the placement of a drain for resolution.2 Most seromas will resolve in 10-14 days. If drained, the fluid usually reforms within 24-48 hours and repeat drainage will increase the risk of ascending infection.
Suture reaction
Most cases of suture reaction are mild and can be left untreated. It is useful to record them as frequent reactions may indicate the suture used is oversized for the patient, that the knot is not buried deep enough in the subcutis. or the suture ends are being left longer than 3 mm.2
Long-term postoperative complications can include a continued mild lameness after an extracapsular suture or urinary sphincter mechanism incompetence (USMI) after ovariohysterectomy.
Recording and auditing long-term complications is perhaps the most difficult step due to the length of time that can pass, the change in personnel, and the updating of recording and auditing systems. However, I encourage you to do what you can to review these. Long-term complications should be looked at in any outcome audit.
Clinical audit
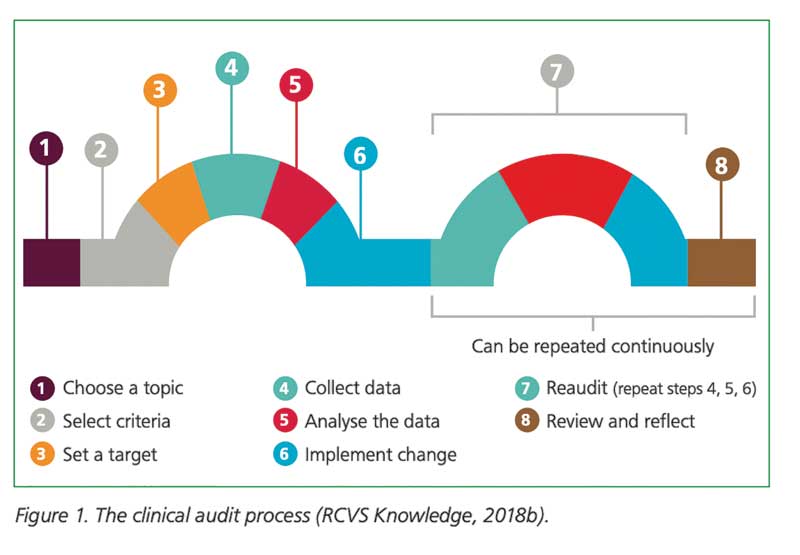
The first step in minimizing complications is to perform an outcome audit.3 The Royal College of Veterinary Surgeons (RCVS) has an excellent toolkit to help you implement and perform a clinical audit in your practice (Figure 1).4 One of the key elements is to appoint an audit lead, and often, a nurse can be best placed to take up this role.3
The changes to implement due to the audit do not have to be radical. When I worked in general practice, the result of our first clinical audit was simply to switch from simple continuous to simple interrupted buried intradermals in our dog castrations. During the audit process, we found an unexpectedly high rate of suture reaction and irritation at the site of the buried knot. Repeating the audit after instituting the new change showed us how effective it was and allowed us to deliver improved patient outcomes and a lower complication rate.
Surgical safety checklist
If you do not already have a surgical safety checklist before and after every single surgical procedure, then I highly recommend you consider adding one. Surgical safety checklists have been proven to reduce mortality and peri- and postoperative complications.5 Each checklist should have three main stages: a sign in prior to anesthesia/surgery, a time out during surgery and, a sign out.6 Someone should be designated the “checklist champion” who ensures the checklist is instituted correctly and stop it from being forgotten. Once you start getting into the routine of “checklisting,” you will find it becomes second nature and everyone in the team will start to prompt the time out/sign out, and not just the “checklist champion.”
One piece of advice I have is make sure to have a consistent strategy intraoperatively for how you handle used sponges. For example, have a target such as a drape on the floor or a single kick bucket that all sponges go into, so it is easy to count before closing. This will prevent errors in accounting for discarded sponges that can lead to a sudden panic as you search the abdomen for the “missing” sponge that has just been discarded into a trash can somewhere.
Support your surgeons
Complications happen to us all and it is important to foster a “positive patient safety culture” in the clinic.7 This is one where everyone accepts that errors occur. It is important for surgeons to seek support after experiencing a major complication, which can be in the form of discussing the technical errors with a colleague, seeking emotional support from family or friends, and sometimes getting professional support from a counselor or therapist.8
When errors happen, an appropriate reprisal-free investigation should be undertaken and the results of this should be shared with the whole team to prevent the same errors from happening again.
In a positive patient safety culture, it is important people feel empowered to question and discuss patient safety issues. Whilst strong unwavering support for unintentional errors is crucial, those within the team should understand it is their responsibility to adhere to policies and procedures that are there to safeguard patient safety.7 As we say in our clinic, each complication is another opportunity to learn, so take the key learning points, treat the patient, and then implement change so it does not happen again.
Jessica McCarthy, BVSc, MRCVS, DECVS, works as a faculty in orthopedic surgery at the University of Wisconsin. Dr. McCarthy became a diplomat of the European College of Veterinary Surgeons in 2020, after completing her residency training at the University of Edinburgh. McCarthy attended Bristol University for her veterinary degree and spent two years in general practice in England after graduating. She has a particular interest in elbow disease, both developmental and traumatic, and is passionate about ensuring everyone in the veterinary profession can work in a diverse and inclusive atmosphere.
References
- Root Kustritz MV. Collection of tissue and culture samples from the canine reproductive tract. Theriogenology. 2006 Aug;66(3):567–74.
- Griffon D, Hamaide A, editors. Complications in small animal surgery. Chichester, UK: John Wiley & Sons, Ltd; 2016.
- Mosedale P. Clinical audit in veterinary practice — the role of the veterinary nurse. Vet Nurs. 2019 Feb 2;10(1):4–10.
- Knowledge, R. (2019, December 2). RCVS Knowledge The Veterinary Clinical Audit Cycle. Belgravia House, 62–64 Horseferry Road London; RCVS Knowledge. Accessed November 1st 2023.
- Abbott TEF, Ahmad T, Phull MK, Fowler AJ, Hewson R, Biccard BM, et al. The surgical safety checklist and patient outcomes after surgery: a prospective observational cohort study, systematic review and meta-analysis. Br J Anaesth. 2018 Jan;120(1):146–55.
- Knowledge, R. (2020, March 2). RCVS Knowledge Surgical Safety Checklist Manual. Belgravia House, 62–64 Horseferry Road London; RCVS Knowledge. Accessed November 1st 2023.
- Hofmeister EH, Love L. Patient safety culture is needed in veterinary medicine. J Am Vet Med Assoc. 2023 Sep 1;1–5.
- Siddaiah-Subramanya M, To H, Haigh C. The psychosocial impact of surgical complications on the operating surgeon: A scoping review. Ann Med Surg (Lond). 2021 Jul 3;67:102530.