 Cutaneous adverse food reaction, also known as food allergy, is an immune-mediated reaction to a food antigen and can be challenging to diagnose. Clinical signs can be non-specific and mimic other conditions. If an adverse food reaction is suspected, how is it diagnosed? What else could be causing these clinical signs? Let’s look at how to successfully diagnose and manage these patients.
Cutaneous adverse food reaction, also known as food allergy, is an immune-mediated reaction to a food antigen and can be challenging to diagnose. Clinical signs can be non-specific and mimic other conditions. If an adverse food reaction is suspected, how is it diagnosed? What else could be causing these clinical signs? Let’s look at how to successfully diagnose and manage these patients.
Defining terms
Food allergy and food intolerance are part of a broader category of conditions called adverse food reactions. They differ from other types of adverse food reactions, such as toxicities and pharmacologic reactions, in that they are instances of an abnormal response to a “normal” food. Here’s a brief snapshot of each:
1) Adverse food reaction is defined as any abnormal clinical response attributed to the ingestion, contact with or inhalation of a food, its derivatives, or an additive contained in it.
2) Food allergy is an immune-mediated reaction, called a hypersensitivity, to an ordinarily harmless substance in food—typically an intact protein.
3) Food intolerance is a non-immune reaction to a wide variety of different dietary components. They include carbohydrates, fats, or dietary additives. It also includes maldigestion or an idiosyncratic reaction, such as a temporary inability to digest a food substance.
Distinguishing allergy from atopy
Patients with a food allergy can have similar clinical signs to patients with atopy, and some patients may even have both. So how do we differentiate between the two? Start with the case history and clinical signs to help us determine our diagnostic protocol.
Food allergy can develop at any age, with clinical signs usually present year-round. Dermatologic signs can include pruritis, erythema and secondary lesions due to self-trauma. Gastrointestinal clinical signs can include vomiting (acute or chronic), diarrhea (acute or chronic), flatulence, frequent defecation, borborygmus, and abdominal pain. If a patient has both GI and dermatologic signs, they are more likely to have a food allergy or the combination of food allergy and atopy.
Atopy is an immediate hypersensitivity reaction to common environmental antigens, including grass, weeds, spores, dust mites, or pollen. Areas of the body most commonly affected by pruritus, erythema and skin lesions include the muzzle, periocular region, ear canals/pinnae, interdigital spaces, axillae, and groin. Atopy also tends to be seasonal. As previously mentioned, it is not unusual for both atopy and food allergy to present in the same patient, so it is important to determine if there is a food component involved—evidenced by year-round dermatologic clinical signs and/or GI signs.
Initiating an elimination diet trial
If a food allergy is suspected, the next diagnostic step is to implement an elimination diet trial—considered the gold standard method of diagnosing an adverse food reaction. In the case of a food allergy, the goal is to eliminate the potential allergen/s from the diet for a period of time to see if clinical signs improve as a result. Here are the steps to prepare for and conduct an elimination diet trial:
Step 1: Obtaining a complete and thorough patient diet history
 To identify potential allergens, it is essential to glean as much information as possible about the dog’s dietary history and everything the dog is eating. This includes food, treats, medications and anything else the dog is ingesting (including eating scraps off the floor). Challenges may arise when obtaining a diet history for a dog that has been adopted from a shelter or has eaten multiple foods (with multiple protein sources) throughout their life. Asking owners to send pictures of the bags of their primary diet(s) and treats can be helpful.
To identify potential allergens, it is essential to glean as much information as possible about the dog’s dietary history and everything the dog is eating. This includes food, treats, medications and anything else the dog is ingesting (including eating scraps off the floor). Challenges may arise when obtaining a diet history for a dog that has been adopted from a shelter or has eaten multiple foods (with multiple protein sources) throughout their life. Asking owners to send pictures of the bags of their primary diet(s) and treats can be helpful.
Step 2: Recording a baseline assessment of clinical signs
Ask the client about the degree of severity of their dog’s clinical signs. The Pruritis Visual Analog Scale (Canine),1 can help document the intensity of a dog’s pruritis. The goal is to establish a baseline of clinical signs in order to track improvement (the goal being improvement of greater than 50 percent).
In addition, the Canine Atopic Dermatitis Extent and Severity Index (CADESI)-42 is a quick visual reference showing 20 body sites typically affected by skin lesions in atopic dogs. For patients with diarrhea, the Purina Fecal Scoring Chart can help clients accurately describe the appearance of their dog’s stools.
Step 3: Work with the client to develop an action plan
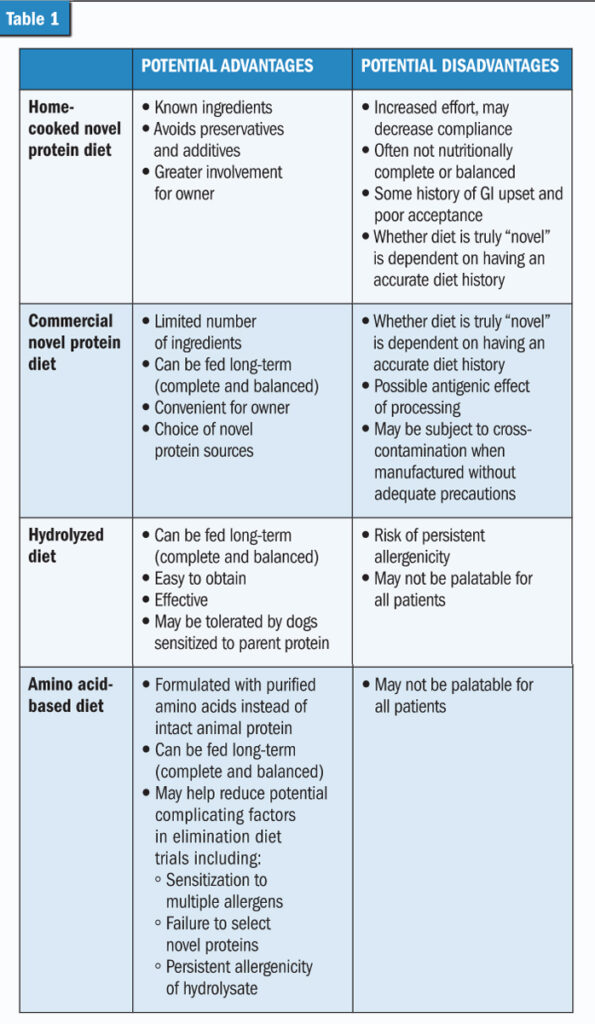
There are four potential types of diets that can be used for elimination diet trials: home-cooked novel protein, commercial novel protein, hydrolyzed, and amino acid-based. This chart can help evaluate these diet options: (See Table 1)
In addition to diet, discuss eliminating other protein sources, such as food supplements, medications, and chew toys and treats that contain animal protein.
If treats are an important part of a client’s relationship with their dog, recommend using part of the main diet as a treat (e.g. reserve some kibble for treats) or have the client home-prepare a single-ingredient treat with the same protein source as the primary elimination diet. Discuss regular clinic check-ins and the timeline in which results may be expected.
Step 4: Implementing the trial
After selecting the elimination diet, practitioners should ensure the client has enough food for a minimum of eight weeks and prepare them for feeding the diet for 16 weeks or longer. The importance of strict compliance and patience to a successful trial should be emphasized.
A slow transition from the dog’s current food to the diet trial food will help ensure that the diet change does not trigger or exacerbate any GI upset. Ideally, the diet should be transitioned over a period of five to seven days, with the ratio of trial diet to original diet gradually increased.
A member of the veterinary team should check in with the client after a week to see how the trial is going, and clients should be encouraged to call the office with questions or concerns. Monthly rechecks can assess patient progress relative to baseline.
The type of clinical signs a dog is experiencing will affect the length of the trial. Dogs with GI signs only typically show improvement in two to four weeks if the cause is diet related. For dogs with dermatologic signs, the diet trial may need to continue beyond 12 weeks if improvement is noted, but is less than 50 percent relative to baseline.
Step 5: Evaluating the situation and rechallenging the patient
If the trial is successful—which is defined as improving dermatologic or GI signs by more than 50 percent—challenge the patient with their old diet to help ensure a component of the diet (typically a protein) was the cause of the clinical signs. This can sometimes be a tough sell to clients (“Why would I want to have my dog deliberately eat the food they’re allergic to?”), but it is essential to achieve an accurate diagnosis of food allergy.
If clinical signs return, talk with the client about continuing long-term management with a complete and balanced hydrolyzed or amino acid-based diet formulated for growth or maintenance of adult dogs (depending on life stage).
If the trial does not improve clinical signs or improvement is less than 50 percent, consider environmental allergy testing, medical treatment, and nutritional management of atopy. The problem could be atopic dermatitis or a combination of food allergy and atopy.
If atopic dermatitis is diagnosed, nutritional management can be used in conjunction with medical management. A diet that includes eicosapentaenoic acid, a beneficial omega-3 fatty acid, can help reduce skin inflammation, help support the skin barrier and reduce water loss via the skin. Essential fatty acids may have a synergistic effect with antihistamines3 and may have a steroid-sparing effect in the treatment of canine atopic dermatitis.4
Allergies can seriously affect quality of life, both for pets and pet owners. With proper diagnosis, nutritional and medical management can provide substantial relief and a path forward to a healthier, more comfortable pet.
|
GETTING TO THE BOTTOM OF IT |
There are several resources that can help with the diet history process, including the following:
|
Jason Gagné, DVM, DACVIM (Nutrition), is a board-certified veterinary nutritionist who serves as director of veterinary technical communications for the Purina Pro Plan Veterinary Diets brand. Dr. Gagné works closely with innovation and renovation, developing clinical trials, and the sales and marketing departments of the brand.
References
- Rybnícek J, Lau-Gillard PJ, Harvey R, et al. Further validation of a pruritus severity scale for use in dogs. Vet Dermatol. 2009 Apr;20(2):115-122. https://pubmed.ncbi.nlm.nih.gov/19171021/
- Olivry T, Saridomichelakis M, Nuttall T, et al. International Committee on Allergic Diseases of Animals (ICADA). Validation of the Canine Atopic Dermatitis Extent and Severity Index (CADESI)-4, a simplified severity scale for assessing skin lesions of atopic dermatitis in dogs. Vet Dermatol. 2014 Apr;25(2):77-85, e25. https://pubmed.ncbi.nlm.nih.gov/24461108/
- Paterson S. Additive benefits of EFAs in dogs with atopic dermatitis after partial response to antihistamine therapy. J Small Anim Pract. 1995 Sep;36(9):389-394. https://pubmed.ncbi.nlm.nih.gov/8583767
- Saevik BK, Bergvall K, Holm BR, et al. A randomized, controlled study to evaluate the steroid sparing effect of essential fatty acid supplementation in the treatment of canine atopic dermatitis. Vet Dermatol. 2004 Jun;15(3):137-145. https://pubmed.ncbi.nlm.nih.gov/15214949/