
Photos courtesy John Lewis
In last month’s column, I discussed the initial details of a memorable patient I cared for 19 years ago: Alice, a two-year-old mixed breed dog, presented to the emergency service of the Veterinary Hospital of the University of Pennsylvania one weekend in November 2004. It was while I was on call for the dentistry and oral surgery service. Alice had unknown trauma while spending time on a large farm in York, Pa.
Presentation
When I examined Alice in the ER, she had a wound on the bridge of her nose, which was slathered in silver sulfadiazine cream. She also had swelling in the caudal right oropharynx, mydriasis and scleral hemorrhage of the right eye, dried blood at the right nostril, and pain upon the slightest opening of the mouth.
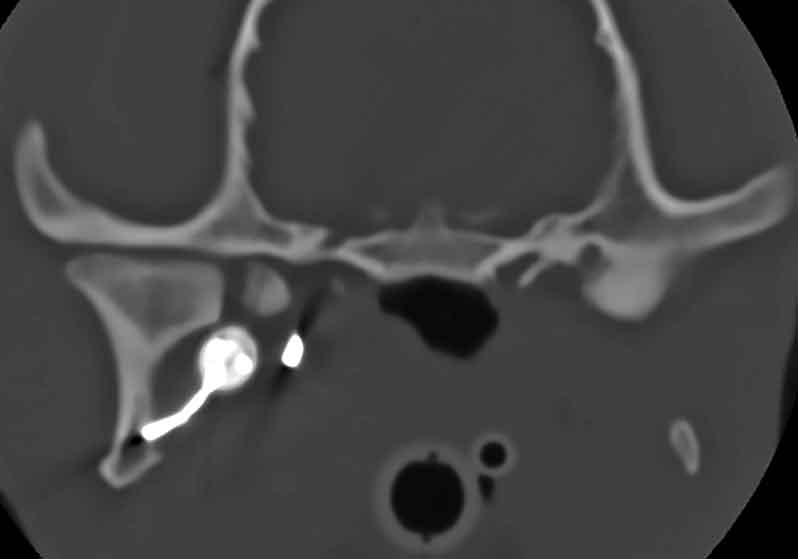
Alice was placed under anesthesia, and radiographs of the head and neck showed a six-inch piece of hunting arrow lodged in her head. After seeing the radiographs, we obtained a CT scan of Alice’s head, which showed exactly how close the blades of the hunting arrow were to severing some of the major vessels in the head. It was amazing Alice survived the impact and did not bleed out on the spot.
The lodged arrow was the type that had three razor-sharp blades. The entry site was obvious after shaving the fur on midline of the bridge of the nose (Figure 1). The site of final impact was at the right mandibular condylar process, where the impact resulted in a condylar fracture (Figure 2). Two of the blades were still attached to the shaft, but one blade dislodged after impacting the medial aspect of the right condylar process.
Surgical plan
After running the imaging tests, we moved Alice to the prep room and developed a surgical plan. Crowds gather quickly around rare cases like this. Steve Mehler, DVM, DACVS, was on call for the surgery service. I asked Dr. Mehler if he had time to scrub in on Alice’s surgery, and he was more than willing despite his packed schedule.
It seemed obvious removing the arrow from its site of entry would cause more harm than good. Therefore, we placed Alice in left lateral recumbency, clipped her face and neck area, and prepped the skin with chlorhexidine and alcohol. We palpated a swelling ventromedial to the mandible in the area of the right mandibular salivary gland. An eight-centimeter incision was made in the neck over the swelling.
Layer by layer, we dissected down to the sharp tip of the arrow (Figure 3A). Using a wire cutter, we removed the two attached blades from the tip of the arrow. Mehler had what I thought was an ingenious idea: attach a Jacobs chuck to the sharp tip of the arrow to allow for a better grasp on it (Figure 3B).
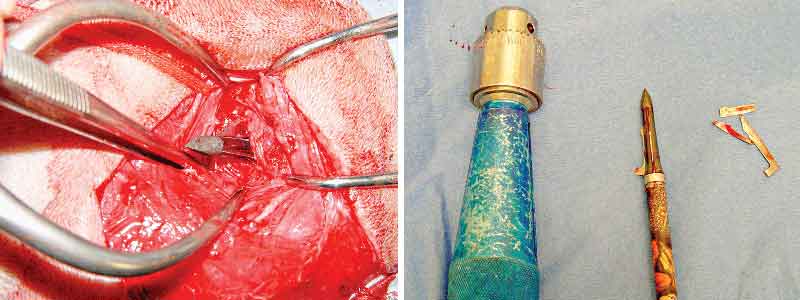
We gently pulled the arrow from the neck, and there was a sudden onset of significant bleeding. A blood transfusion was started, and the source bleeding was identified and ligated.
The third blade of the arrow proved challenging to find within all the swelling, so we decided to leave it and attempt to remove it in the future once the swelling resolved. We chose to pursue no treatment of the fractured right condylar process. We measured Alice’s range of jaw motion prior to waking from anesthesia, and found there was still a slight decrease in the ability to fully open the mouth compared to normal, which was attributed to either the remaining piece of metal or the condylar fracture. We warned the owner that possible TMJ ankylosis or pseudoankylosis might result in an even further decrease in range of motion in the coming weeks and to monitor for evidence of this at home.
Recovery
Alice recovered from anesthesia in the ICU overnight. When I returned the next morning, she was standing at the front of her run, with her now classic (and unrelenting) tail wag.
Alice was discharged into the care of her owner, Charlotte. I handed Charlotte a bag containing the arrow and all the retrieved pieces, which she provided to the York Police with hopes that Alice’s perpetrator(s) could be found. The optimist in me wanted to hope that Alice’s wound was a case of mistaken identity (a large fox?), but the “right between the eyes” nature of the wound suggested this arrow was shot from point blank range.
Alice continued to do well at home and was rechecked at two and four weeks, postoperatively. At the four-week postoperative visit, it was noted that previous mydriasis due to suspected optic neuritis had resolved (Figure 4). We placed Alice under anesthesia for further assessment and possible removal of the final blade of the arrow. The caudal oropharynx, skin over the nose and neck, had healed nicely. Swelling in the neck region had resolved. Range of motion was still slightly decreased compared to normal.

Alice was placed under anesthesia. David Holt BVSc, DAVDC, utilized a ventral approach to the right TMJ area, making a challenging retrieval of the final blade seem easier than it really was (Figure 5). A small Penrose drain was placed medial to the incision and removed after four days. Alice’s range of motion immediately improved after removal of the final blade.

The doctors and nurses of no less than eight specialty services worked together to allow Alice to survive, including Emergency, Radiology, Surgery, Dentistry/Oral Surgery, ICU, Transfusion Medicine, Ophthalmology, and Neurology.
Alice’s story is one of unexpected survival in the face of extreme adversity. It is remarkable she did not die upon impact due to hemorrhage or shock. In the ER, her tail was literally wagging as she greeted each visitor to the front of her run, while she had an arrow buried in her head!
We have all heard of studies from human healthcare of how mindset of the patient affects medical outcomes. I have no doubt that Alice’s demeanor allowed her to survive the initial hours of confusion and severe pain. It is also impressive that Alice’s tail continued to wag for each human she encountered, despite multiple negative experiences while in the care of humans, such as the initial trauma and surgeries.
Although I lost contact with Alice and Charlotte a year or two later, I would like to think Alice lived to a ripe old age. Alice was an inspiration to everyone who met her, and she continues to teach us lessons decades later.
John Lewis, VMD, DAVDC, FF-OMFS practices and teaches at Veterinary Dentistry Specialists and Silo Academy Education Center, both located in Chadds Ford, Pa.