Adequate pain management, according to the 2015 AAHA/AAFP Pain Management Guidelines for Dogs and Cats, brings an overall improvement in surgical outcomes. Besides increasing patient comfort, adequate pain control has other benefits, including faster healing times, less patient interference with the surgical site, and reduced chance of the development of a chronic pain syndrome, such as allodynia.
During surgery, pain management can also help lower the need for elevated anesthesia levels, which can increase the risk of anesthetic-related adverse events. Surgery times may be impacted on animals that have physical responses to the pain, delaying whatever procedure may be performed.
Additionally, surgical patients with good pain control can have procedures done with little or no tie-down restraint, decreasing the chance of injury to limbs held in abnormal positions.
Local anesthetics are the only analgesic we use, everything else is hypoalgesic. Drugs, such as lidocaine and bupivacaine, have the ability, when properly administered, to block 100 percent of surgical pain. Although other drugs, such as opioids, are useful and have an important place in sedation and pain control, they only partially block pain impulses. Luckily for us, sodium channel blockers (e.g. lidocaine) are inexpensive, easy to use, and safe when following dosing and administration guidelines. The other benefit is they have applications for the most common procedures done by general practitioners: neuters, spays, and lumpectomies.
Testicular blocks
Testicular blocks are very easy to perform. In my clinic, they are performed by a veterinary technician or nurse. When doing them in dogs, they require one extra step: to block the incision site. This is not needed in cats as the testicle is removed through a scrotal incision. Given this area is very vascular, it is important to use lidocaine, not bupivacaine, as the risk of injecting into the blood stream is higher.
Whether you are performing a testicular block in a dog or a cat, the first step is to make sure you have a needle long enough to reach the cranial pole of the testicle. Generally, I use a 22-gauge needle of varying lengths for dogs, and a 23-gauge ¾-in. needle for cats (Figure 1).

The next step is to swab the testicle with alcohol, prior to the injection. At this point, the needle is inserted through the caudal pole of the testicle, stopping just before leaving the cranial pole of the testicle (Figure 2). Then, while firmly grasping the testicle, start to inject only until you just start to feel some pressure. If this is a cat, you are done. If it is a dog, you now need to use the needle to perform a line block over the incision site (Figure 3).


In the time it takes to finish prepping the surgery site, the lidocaine will have had its full effect.
Some people prefer to perform a block directly into the vas deferens, but it is a smaller target, requires a better grasp of the anatomy, and, in the end, the lidocaine in the testicular injection makes its way to the vas deferens.
It is also not unusual to find some minor bleeding has occurred as a result of the testicular injection. This is almost always minor, and when the testicle is surgically removed, it resolves the bleeding.
Ovarian blocks
An ovarian block is easier to do, but needs to be performed by the surgeon as it is done directly into the ovarian ligaments.
A small amount of lidocaine must be drawn up into a syringe observing sterile technique. This is done by sterile placement of a 3-cc syringe, usually with a 22-gauge needle on it, onto the surgery pack. The surgeon then inserts the needle into the bottle of lidocaine, the assistant turns the bottle upside down, and a cc or so of lidocaine is drawn up in the syringe and the needle is removed from the bottle.
Once the ovary is exteriorized from the abdomen, the rest is easy, avoiding any obvious blood vessels, passing the needle through the fatty ligaments between the ovary and the ligament attachment. As you slowly withdraw the needle, dribble several drops of lidocaine until the needle is completely out. This does not seem like much, but for most cases this is enough to block some, if not all, of the nerves (Figure 4).

At this point, I do one of two things. As the lidocaine takes about three minutes or so to work, I will drop the ovary back into the abdomen, exteriorize the other ovary, repeat the procedure, then drop it into the abdomen and pull out the first ovary, which should now be blocked. However, if it took me more than three minutes to find the first ovary, then I will wait out the three minutes then clamp and cut that side before going to the second ovary.
Occasionally, especially in dogs with very fatty ligaments, I will hit a blood vessel. If that happens, I do not drop the ovary back into the abdomen, but instead will clamp the ligament proximal to the point of bleeding and perform the ovariectomy without waiting for the lidocaine to take effect. This does not happen often, but when it does, I have to forgo the benefit of a blocked ovary.
Lumpectomies
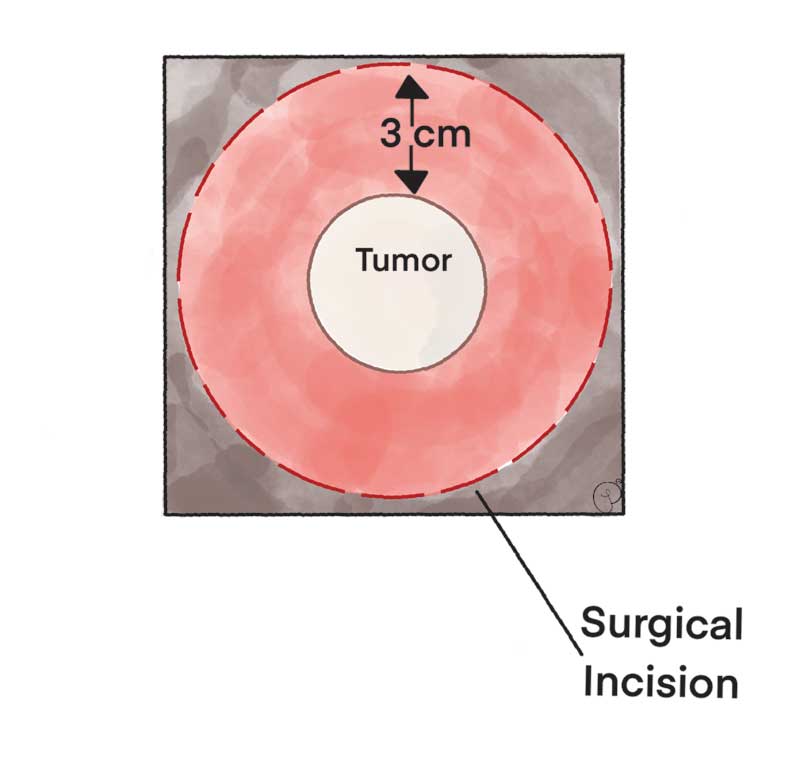
Removing lumps, whether benign, cancerous, or cystic, is one of the more common surgeries performed in general practice. Very small lumps, such as sebaceous adenomas, can be blocked by basically performing a line block that extends under the lump. Larger lumps can be blocked by imagining the lump at the base of an inverted pyramid. The other consideration is if this is a growth that might be malignant, then the base of the pyramid should encompass a 3-cm margin around the potential tumor (Figure 5).
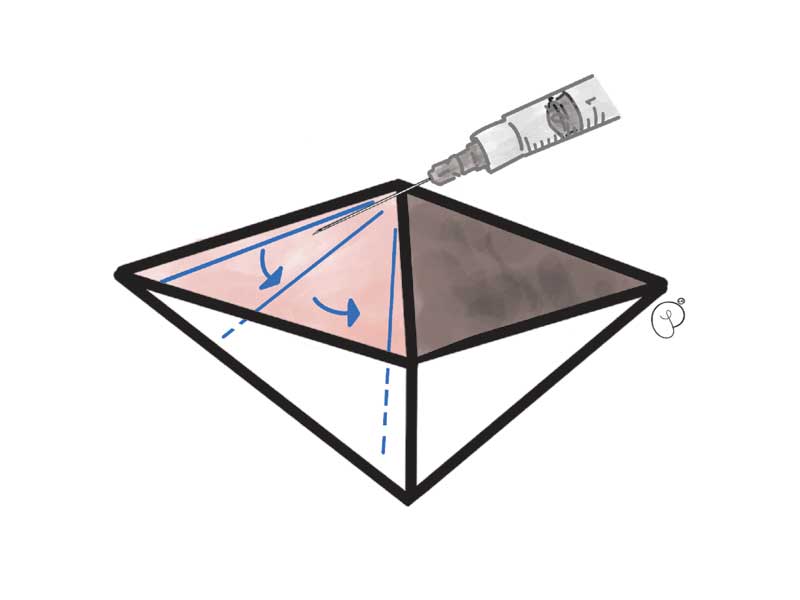
Imagine a four-sided inverted pyramid with the proposed incision lines at the outer base of the pyramid. On one corner of the pyramid, there will be a total of five injections of lidocaine or bupivacaine. The first one will start as a line block under the surface of the skin, extending from the adjacent point on the pyramid and injecting as you withdraw to the insertion point. Without completely removing the needle, you will then inject along the side of one face of the pyramid, and then under the lump from the apex of the pyramid. Continue the injections by moving in the same direction, but in the opposite order by injecting along the side of the next face of the pyramid and then along that edge for another line block.
Next, insert the needle opposite from the original insertion point at the base of the imaginary pyramid, and repeat the five injections as above. At this point you will have effectively blocked the entire growth (Figure 6).
Depending on the size of the lump, it is sometimes hard to effectively cover all injection points with a safe dose of local anesthetic. You can increase the volume by diluting the lidocaine or bupivacaine half and half with saline. The block will still be complete; however, it will only last half as long.
Another trick is to start with bupivacaine and finish with lidocaine if you run out. The toxic doses of lidocaine and bupivacaine are not additive; therefore, you can use a full dose of each at the same time.
Finally, I always start my injections on the side I know the nerves are coming from. It is helpful for me to imagine that the dog or cat has zebra stripes, which run from the top midline downward, in the same way that nerves come off the spinal cord. In this manner, you may have a very effective block of most of the nerves even if you do not have enough to inject into the ventral side of the circumference.
Diffusion catheters
Occasionally, we are faced with very large growth removals, such as lipomas, that are going to be quite painful in the days following the surgery. When that is the case, I like to place a diffusion catheter in the surgical site prior to close.
You can buy commercially available catheters, but they are easy to make, as well. The benefit of making your own is they are inexpensive and can be tailored to the exact size of the area that needs to be covered. The procedure takes just a few minutes and can be done right at the end of the surgery prior to closing.
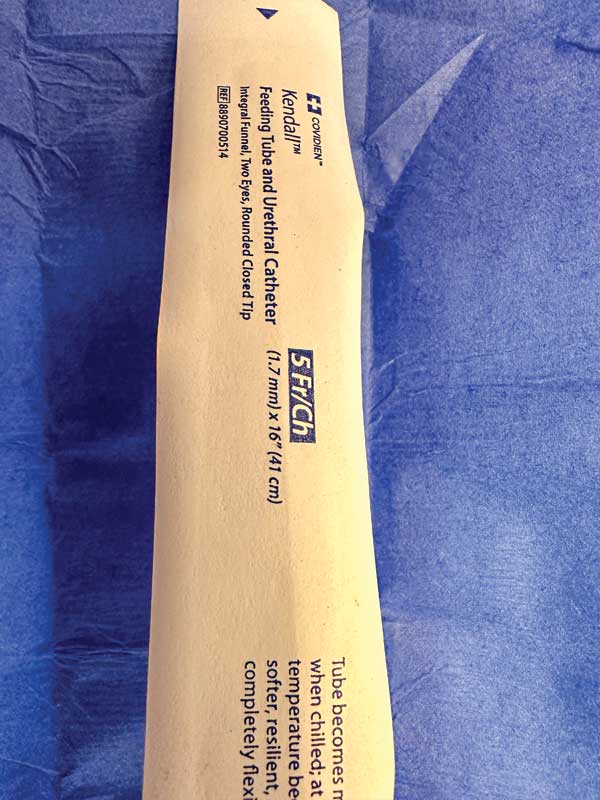

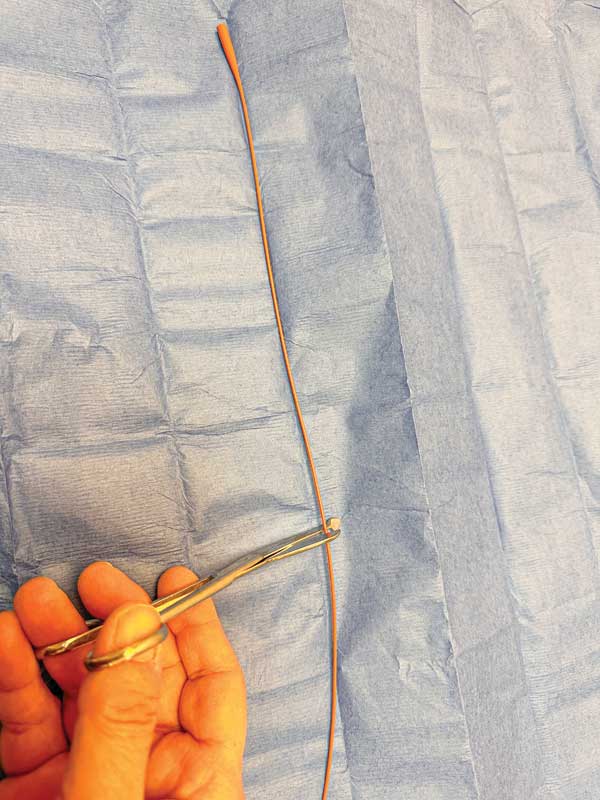
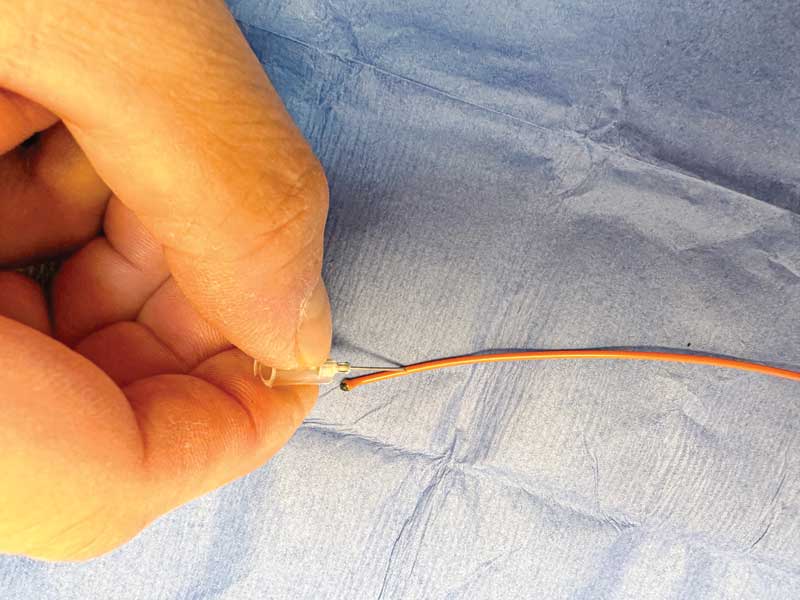
I like to use #5 French feeding tubes/urinary catheters (Figures 7 and 8). The first step is to cut it to size after determining the length needed to go from the skin to the farthest edge of the incision (Figure 9). The cut end must then be sealed to prevent the anesthetic from coming out as that is the path of least resistance and the fluid would pool at the end of the catheter. This is done by briefly having an assistant hold a flame under the tip of the catheter, and then using several layers of gauze to pinch the melted end shut. Use enough gauze to protect yourself from a burn (Figure 10).

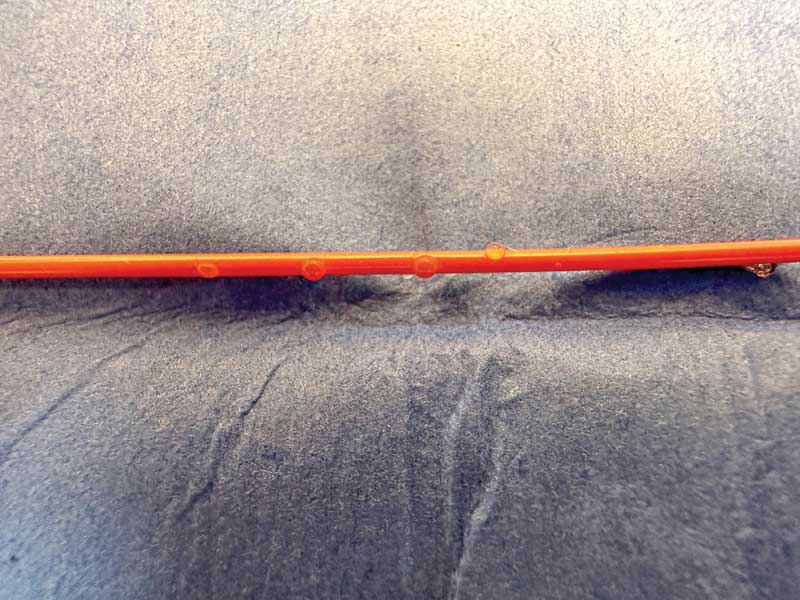
Now it is time to make the perforations. I generally use a 22-gauge needle to make holes every 5 mm or so apart for the length needed to cover the surgical area. (Figure 11). You now have a diffusion catheter capable of delivering anesthetic to the surgery site (Figure 12).
Both lidocaine and bupivacaine come in preserved and non-preserved forms. I prefer the preservative-free forms for diffusion catheters as the preservative can sting on injection. However, it is possible to add 0.1 ml of injectable sodium bicarb to each ml of preserved anesthetic. You will see a small precipitate form, but this is the preservative, and the presence of the precipitate does not alter the effectiveness of the anesthetic.
|
VPN Plus+ members can view clips of these |
Michael Petty, DVM, is a graduate of the veterinary school at Michigan State University. As the owner of Arbor Pointe Veterinary Hospital and the Animal Pain Center in Canton, MI, Dr. Petty has devoted his professional life to the care and well-being of animals, especially in the area of pain management. Petty is the past president of the International Veterinary Academy of Pain Management. A frequent speaker and consultant, he has published articles in veterinary journals and serves in an advisory capacity to several pharmaceutical companies on topics of pain management. Petty has been the investigator/veterinarian in 12 FDA pilot and pivotal studies for pain management products. He has lectured both nationally and internationally on pain management topics.