
Diabetes mellitus (DM) is a common disease that affects the body’s ability to convert glucose into energy as a result of an absolute or relative insulin deficiency.1 According to recent studies, the prevalence of DM today is one in 230 cats2 and one in 308 dogs.3 This is a marked increase over what it was just 10 years prior to this study, which was performed in 2016.4
Insulin deficiencies can be due to decreased insulin secretion or the inability of cells to react to the insulin that is present.1 It is crucial to understand and to convey to pet owners at every opportunity that regardless of the cause, with proper management, a diabetic dog or cat can lead an otherwise normal and active life.
Types
Two types of DM are recognized in both human and veterinary medicine. Type I diabetes is a relative or complete lack of insulin secretion. In human medicine, this is considered juvenile diabetes. This is the most common type in dogs and almost always requires insulin therapy.
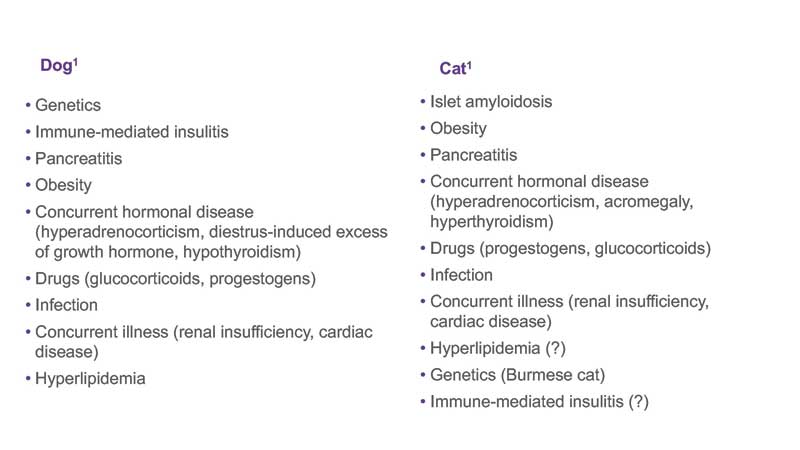
Type II diabetes is a lack of insulin efficacy due to the inability of the cell to bind or properly respond to insulin, often called insulin resistance. This type is most common in older adult humans and is thought to be more common in cats. Several risk factors are associated with diabetes in both cats and dogs. (Table 1)
Unlike in human medicine, most cats suffering from type II diabetes require insulin therapy. Therefore, a functional distinction of insulin-dependent diabetes mellitus (IDDM) and non-insulin-dependent diabetes mellitus (NIDDM) is more useful in veterinary medicine than the traditional human type I and type II designations.
Common clinical signs in both dogs and cats can include:1, 5
- Fatigue or weakness. Sleeping more than usual, acting sluggish or less playful, appearing sick or not feeling well, poor body or coat condition
- Increased hunger. Eating more, but has not gained weight
- Excessive thirst
- Frequent urination
- Weight loss is common despite the increased appetite
Additional clinical sequelae can include neuropathies or dropped hocks in cats, and cataract formation in dogs.1,4
Diagnosis
The diagnosis of DM is made by documenting persistent hyperglycemia and glucosuria, with presence of clinical signs of polyuria, polydipsia, polyphagia, and weight loss. The following diagnostics should be considered:1, 5
- Complete blood count
- Serum biochemical panel
- Urinalysis with bacterial culture
- Progesterone in intact female dogs
For dogs: If available, abdominal ultrasound to assess for pancreatitis, adrenomegaly, pyometra (intact female dog), and liver and urinary tract abnormalities (pyelonephritis or cystitis).
For cats: abdominal ultrasound to assess for pancreatitis and evaluate adrenal glands. Pancreatic lipase immunoreactivity (cPLI) in dogs and pancreatic lipase activity (fPLI/Spec fPL) in cats to test for pancreatitis, especially if no ultrasound available. - Serum thyroxine (T4).
Treatment
Following the often relatively straightforward diagnosis of DM, treatment should be instituted without delay. Left untreated, additional complications of DM can occur, such as deterioration to the catabolic state of ketoacidosis. This is especially true when the DM is complicated with additional common inflammatory or infectious disorders, such as pancreatitis or urinary tract infections. It is crucial for the veterinary staff to convey the realistic goals of treatment to the pet owner.1,5,6 (Table 2)

Unlike in human medicine, where strict glycemic control is necessary to prevent long-term DM sequelae, such as vascular, cardiac and renal disorders, veterinary patients tolerate much wider swings in glucose concentrations throughout the day with no long-term effects. Thus, our goal is to minimize clinical signs, avoid hypoglycemia and provide our patients and their owners with a normal happy life and not to have perfect glucose measurements 24 hours a day.
This understanding is important since the diagnosis can be overwhelming for the pet owner and the initial tendency to euthanize is very common. This conversation must occur with the pet owners prior to the next step—teaching them how to administer insulin.
Administering insulin
Teaching the owners about insulin and how to administer it is likely the most important part of the management of diabetes, and should be done slowly and over time—often best by a veterinary technician, a DM champion who is trained and has become experienced in facilitating the DM management team that consists of the owner, veterinary technician and veterinarian.
The initial fear of giving injections can be overcome in almost every case by patient, but with persistent coaching and lots of practice on objects such as oranges. The owner should also practice gently rolling (not shaking) and then drawing up the insulin in an insulin syringe—the exact same type that will be sent home.
Patient monitoring
Unless the patient is systemically ill (diabetic ketoacidosis [DKA], pancreatitis, hepatic lipidosis etc.) it is not recommended to try and regulate insulin dose in the hospital. Dogs and cats should be sent home on a conservative initial dose and instructed to come back in for a recheck in one to two weeks, when the monitoring phase of the management begins.
Continuous glucose monitors can be used in this initial period but are often not deemed necessary in most patients. At this recheck, it is often the best time to start the conversations about long-term monitoring of the patient, ideally more at home than in the clinic as at-home blood glucose monitoring is much more reflective of the pet’s true environment than the stress-induced glucose levels that are captured during a clinic visit.6
In addition to glucose concentrations, serum fructosamine can be measured in the clinic. Urine should be monitored for ketones when there is a question of the pet being ill or for repeated negative results when there is a possibility of too much insulin being administered but should not be used for glycemic control assessment or insulin dose calculations. Monitoring of capillary blood glucose should always be done with a veterinary glucometer validated for the species it is being used on, as specific algorithms are necessary for interpreting the capillary glucose concentrations in every species.
The benefits of at-home monitoring with a validated veterinary glucometer include:6
- Helps assess effectiveness of current treatment program
- Provides data to enact changes to optimize treatment plan
- Reduces potential stress hyperglycemia associated with hospitalizations, especially in cats
- Readings obtained in the pet’s everyday environment may be more reflective of the true blood glucose value
- Can more readily monitor changes in blood glucose based on activity, diet, etc.
It is very important the pet owner be able to share the information with the veterinary staff and that all insulin dose decisions are made by the veterinarian and not by the pet owner, except for the standing instruction to skip the insulin and call if the pet is ill or will not eat. The owner should always ensure the pet is eating prior to administering the insulin dose that is due.
Spot glucose checks can be helpful, especially if taken at the same time of day to notice trends, but glucose curve should be performed periodically to verify the correct insulin and dose are being used. These curves are much better done at home, but if not possible, can be done in the clinic as well in some cases, especially in dogs.
Blood glucose (BG) curves performed in the veterinary clinic almost never yield helpful results in cats because of stress hyperglycemia associated with hospitalization.6 Glucose measurements are typically taken every two hours for eight to 12 hours. The curve has the following benefits:6
- Provides important information for adjusting insulin therapy.
- Displays information about insulin dose (under/over) and duration of current insulin therapy.
- Provides important data for initial blood glucose regulation, or in situations where clinical manifestations of hyperglycemia or hypoglycemia have occurred.
However, measurements from blood glucose curves must always be interpreted in light of clinical signs, results may vary from day to day and can be affected by deviation from the patient’s normal routine and as stated above, especially in cats, results can be unreliable in stressed, aggressive or excited animals.
Serial glucose curves should be performed seven to 14 days after an insulin dose has been increased or decreased, or a new insulin type has been started, to identify hypoglycemia if suspected, at any point in time if clinical signs recur in a controlled patient and periodically in a well-controlled diabetic patient (at least once every three months).
A normal insulin treatment and feeding schedule must be maintained as much as possible while obtaining a BG curve. A BG curve should establish duration of treatment effect and the lowest BG (i.e. the nadir).6
- The ideal nadir is a BG of 80-150 mg/dL (4.4- 8.3 mmol/L)
- The highest BG should be close to 200 mg/dL (11.1 mmol/L) in dogs and 300 mg/dL (16.7 mmol/L) in cats
When interpreting the BG curves, the veterinarian should ask these to make proper decisions on changes to insulin type, dose, and frequency:
- What is the nadir?
Has the insulin succeeded in lowering BG to an ideal nadir of 80–150 mg/dL (4.4- 8.3 mmol/L)? - What was the duration of action of the insulin?
How long has the BG been controlled between 80 – 200 mg/dL (4.4- 11.1 mmol/L) in dogs or 80 – 300 mg/dL
(4.4- 16.7 mmol/L) in cats? - Are clinical signs of hyperglycemia or hypoglycemia reported?
In general, the BG curve helps determines the nadir and the duration of action of the insulin being administered.
In summary, a DM diagnosisis not and should not be a death sentence. For diabetic dogs and cats, establishing a DM team made up of the veterinarian, the vet technician, and the pet owner is crucial to the success of
the program.
Appropriate client communication and coaching along with veterinary intervention with proper diagnosis, management, and monitoring can produce successful outcomes, and pets can lead active lives. In-clinic monitoring options include performance of BG curves, monitoring urine glucose, measuring fructosamine, and assessment of clinical signs and weight. At-home monitoring is strongly recommended. Obtaining a blood glucose curve is particularly recommended for cat owners to avoid stress hyperglycemia in a hospital setting.
Richard E Goldstein, DVM, DACVIM (SAIM), DECVIM-CA graduated from the Koret School of Veterinary Medicine, The Hebrew University of Jerusalem, Israel in 1993 and completed a residency in Small Animal Internal Medicine at the University of California (UC), Davis in 1998. Dr. Goldstein served as an associate professor then associate professor with tenure at Cornell University, College of Veterinary Medicine from 2001-2012. In 2012, Goldstein joined the leadership team of the Animal Medical Center in New York City as chief medical office and served in that capacity until January 2018. In 2018 Dr. Goldstein joined Zoetis and is currently the vice president and chief medical officer of Global Diagnostics.
References
- Nelson RW. Canine diabetes mellitus. In: Feldman EC, Nelson RW, Reusch CE, Scott-Moncrieff JCR, editors. Canine and feline endocrinology. 4th ed. St. Louis: Saunders Elsevier; 2015. p. 213-257
- McCann TM, Simpson KE, Shaw DJ, Butt JA, Gunn-Moore DA. Feline diabetes mellitus in the UK: the prevalence within an insured cat population and a questionnaire-based putative risk factor analysis. J Feline Med Surg. 2007 Aug;9(4):289-99
- Catchpole B, Ristic JM, Fleeman LM, Davison LJ. Canine diabetes mellitus: can old dogs teach us new tricks? Diabetologia. 2005 Oct;48(10):1948-56.
- State of Pet Health 2016 Report – what diseases are affecting dogs and cats (Internet). Banfield Pet Hospital; 2016 (cited July 25, 2023). Available from: https://www.banfield.com/en/pet-health/State-of-pet-health.
- Reusch CE. Feline diabetes mellitus. In: Feldman EC, Nelson RW, Reusch CE, Scott-Moncrieff JCR, editors. Canine and feline endocrinology. 4th ed. St. Louis: Saunders Elsevier; 2015. p. 258-314.
- Behrend E, Holford A, Lathan P, Rucinsky R, Schulman R. 2018 AAHA Diabetes Management Guidelines for Dogs and Cats. J Am Anim Hosp Assoc. 2018 Jan/Feb;54(1):1-2
- Reineke EL. Blood glucose monitoring and glycemic control. In: Creedon JM Burkitt, Davis H, editors. Advanced monitoring and procedures for small animal emergency and critical care. Hoboken, New Jersey: John Wiley & Sons; 2012. p. 776-788
- Gostelow R. Top 5 maintenance insulins. Clinician’s brief [Internet]. 2015 Nov (cited 2023 Aug 10); Available from https://www.cliniciansbrief.com/article/top-5-maintenance-insulins