Anatomy review
There are two cruciate ligaments in the dog and cat, known as cranial and caudal. Each ligament has two separate components. The two components of the cranial cruciate ligament can be easily visualized in the normal patient as two distinct bands.1 The two bands of the caudal cruciate ligament are less distinct but can be visualized using the magnification provided by arthroscopy. The cranial cruciate ligament prevents cranial tibial drawer, hyperextension of the stifle, and limits internal rotation of the tibia. The caudal cruciate ligament prevents caudal tibial drawer.
Presenting signs
Cranial cruciate ligament disease is the most common cause of lameness in dogs and is occasionally seen in cats.2 The degree of lameness on presentation can vary with the stage of disease, the degree of instability, the stage of secondary osteoarthritis, and whether there is concurrent meniscal pathology.
One of the early signs of cranial cruciate ligament disease in dogs is reduced weight bearing through the affected limb at stance. This is often noticed by owners as “offloading” of the limb when their dog is standing at the food or water bowl. Due to swelling of the stifle joint, many dogs splay their legs to the side when sitting to avoid fully flexing the swollen, painful stifle (Figure 1).

Partial cranial cruciate ligament rupture
Partial cranial cruciate ligament rupture can occur in dogs. This is usually due to a rupture of one of the two components (or bands) of cranial cruciate ligament, most often it is the craniomedial band.3 To detect a partial tear, the cranial drawer should be tested in flexion.
The cranial drawer will be positive in flexion only and not present when the stifle is extended. This is because the caudolateral band of the cranial cruciate ligament is only taut with the stifle in extension, and this will prevent cranial drawer when it is still intact. With the stifle held in flexion, the caudolateral band is slack and will not limit cranial drawer and, therefore, with rupture of the craniomedial band, cranial drawer will be present.
It is recommended to perform this with the patient sedated as testing the cranial drawer with a partial cranial cruciate ligament rupture can be painful since the intact caudolateral band is often inflamed leading to discomfort when stretching the ligament.
Partial cranial cruciate ligament rupture has been rarely reported in cats and should still be considered a differential diagnosis when pain and inflammation is localized to the stifle.4
Diagnosis
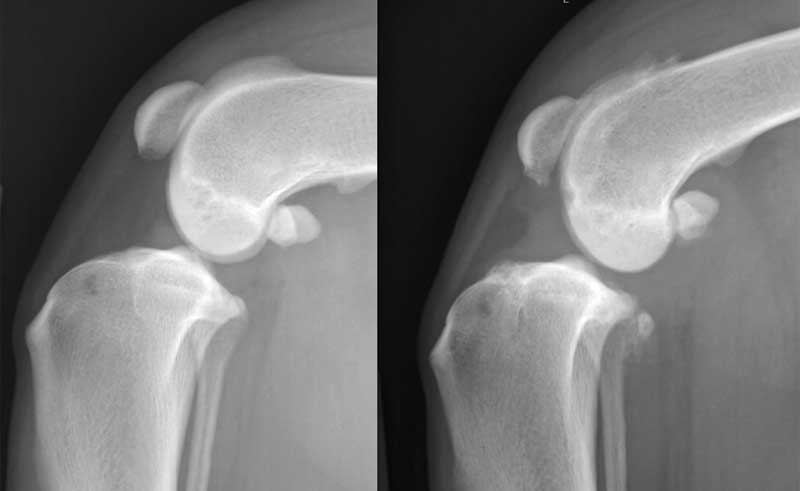
Complete certainty of the diagnosis of cranial cruciate ligament rupture can usually only be achieved via an arthroscopic or direct examination of the ligaments. However, cranial translation of the intercondylar eminences relative to the femoral condyles on a straight lateral radiograph (Figure 2), combined with palpation, will provide reasonable confidence in the diagnosis.5
In cats, there may be mineralization of the meniscus evident as irregular radiopaque intra-articular material on a lateral stifle radiograph. Large mineralization can be associated with cranial cruciate disease and whilst smaller mineralized bodies are more often associated with general age-related osteoarthritis.6
Management of cranial cruciate ligament rupture
Medical management of cruciate ligament disease fails to address stifle instability, which will lead to progressive osteoarthritis that can be severe and debilitating, particularly in overweight animals that are bilaterally affected.
Surgical stabilization of the stifle requires the placement of implants, which can range from monofilament nylon, braided non-absorbable suture, titanium cages, or stainless-steel plates and screws. Surgical site infection occurs in six to 17 percent of cranial cruciate ligament surgeries leading to implant removal in around 50 percent of these cases and resulting in worsened outcomes for
these patients.7
Considerations for patients with skin disease
Due to the high risk of surgical site infection in patients undergoing surgery for the management of cruciate disease, the skin surrounding the surgical site should be carefully inspected prior to anesthesia and again after clipping (Figure 3).

Pre-surgical treatment
If pyoderma is present, then this is treated prior to proceeding with the surgery in an attempt to substantially reduce the risk of surgical site infections (SSI). Treating the pyoderma will vary depending on the severity, the suspected organism, and the dermatological history of
the patient.
Cytological evaluation of a pustule is recommended to confirm the presence of bacteria, to determine whether they are rods and/or cocci, and to roughly quantify the number of bacteria present. If the patient is anesthetized at the time of recognition of the pyoderma, then often a small biopsy of one of the pustules can be taken and submitted for culture and sensitivity.
If the pustules are noticed prior to anesthesia, then a representative sample from a pustule is submitted on a swab for culture and sensitivity testing.
Topical and oral treatments
Pre-surgical treatment of pyoderma will vary from topical treatment only, to topical combined with oral antibiotics. The length of treatment will also vary depending on the severity of the pyoderma. The goal is to eliminate the presence of bacteria prior to surgery, which should be confirmed by cytology, particularly if some papules are still present.
For cases that require oral antibiotics for pre-surgical resolution, we usually continue a short course of antibiotics postoperatively in an attempt to limit their risk of developing an SSI. Usually, this will be a two-week postoperative course, but can vary from patient to patient.
For patients with chronic skin disease but without a pyoderma, we will sometimes recommend owners apply a topical chlorhexidine containing mousse on the surgical site and surrounding area for a couple of days prior to the surgery to try to minimize the risk of SSI.
Such topical treatment may also be useful for patients with a history of colonization with methicillin-resistant bacteria.
Many patients with skin disease receive oclacitinib maleate for control of their pruritus. There is an increased risk of SSI for patients receiving oclacitinib maleate, but this must be balanced with a worsening skin barrier if the patient starts to become pruritic again.8 In our clinic, we usually stop the medication a couple of days before and after the surgical procedure, but this can vary depending on the severity of the skin disease. Further research is required to determine the best practice on how to reduce the risk for SSI for patients with skin disease who are receiving oclacitinib maleate.
Surgery preparation
During surgical site preparation in patients with dermatological disease, be careful in monitoring the patient’s response to chlorhexidine, and prepare to switch to an iodine-based surgical solution if signs of irritation appear.
Additionally, you may take extra precautions, such as double gloving, prior to draping in. Once the skin is completely covered with an iodine-impregnated drape, remove the outer pair of gloves. If a multifilament non-absorbable material is to be used, change all gloves prior to handling the material and do not let the material come in contact with the patient’s skin under any circumstance.
Post-surgical care
Postoperative antibiotics for 10-14 days are given to most patients that have a multifilament nonabsorbable implant placed regardless of whether that patient has dermatological disease.
Intraoperative antibiotics are indicated for any patient undergoing a sterile orthopedic procedure with the placement of permanent implants. There is conflicting evidence regarding the use of postoperative antibiotics and their effect on SSI in elective orthopedic procedures, and further studies are needed to provide best practice recommendations.9
A course of postoperative antibiotics may lessen the number of SSIs but those that occur will likely have a higher likelihood of being methicillin-resistant infections and, therefore, the risks of this should be carefully considered.
Intraoperative antiseptic lavage has not yet been shown to help reduce SSI, with a recent study showing a higher rate of SSI in those patients.10
In our hospital we place a nonadherent dressing over the surgical site in a sterile fashion prior to undraping that will remain in place for a minimum of 12 hours postoperatively, but for no more than 24 hours. Once this dressing is removed, if the patient has dermatological disease, we will often discharge them with an antiseptic wound spray containing hypochlorous acid to be applied two to three times daily to the surgical site and surrounding skin. Hand hygiene before and after touching every patient is required and gloves are used as an adjunct to this but not as a replacement.
Conclusion
Due to the increasing number of drug-resistant bacteria and the lack of evidence-based support for postoperative prophylactic antibiotic use, it is important to carefully evaluate the skin prior to surgery. The aim is to perform surgery on the healthiest skin possible for the patient to reduce the risk of SSI.
Finding an underlying cause for any dermatological disease and addressing it, such as food allergy, is considered the most effective treatment. Topical treatment is preferred where possible, but sometimes the severity of the infection and the necessity for surgical treatment mean oral antibiotics are required. Attention to hospital and patient biosecurity protocols are paramount in reducing SSI, particularly in at-risk patients undergoing elective procedures.
Jessica McCarthy, BVSc, MRCVS, DECVS, works as a faculty in orthopedic surgery at the University of Wisconsin. Dr. McCarthy became a diplomat of the European College of Veterinary Surgeons in 2020, after completing her residency training at the University of Edinburgh. McCarthy attended Bristol University for her veterinary degree and spent two years in general practice in England after graduating. She has a particular interest in elbow disease, both developmental and traumatic, and is passionate about ensuring everyone in the veterinary profession can work in a diverse and inclusive atmosphere.
References
- de Rooster H, de Bruin T, van Bree H. 2006. Morphologic and functional features of the canine cruciate ligaments. Vet Surg. 35(8):769–780. doi:10.1111/j.1532-950X.2006.00221.x.
- Taylor-Brown FE, Meeson RL, Brodbelt DC, Church DB, McGreevy PD, Thomson PC, O’Neill DG. 2015. Epidemiology of Cranial Cruciate Ligament Disease Diagnosis in Dogs Attending Primary-Care Veterinary Practices in England. Vet Surg. 44(6):777–783. doi:10.1111/vsu.12349.
- Scavelli TD, Schrader SC, Matthiesen DT, Skorup DE. 1990. Partial rupture of the cranial cruciate ligament of the stifle in dogs: 25 cases (1982-1988). J Am Vet Med Assoc. 196(7):1135–1138. doi:10.2460/javma.1990.196.07.1135.
- Mindner JK, Bielecki MJ, Scharvogel S, Meiler D. 2016. Tibial plateau levelling osteotomy in eleven cats with cranial cruciate ligament rupture. Vet Comp Orthop Traumatol. 29(6):528–535. doi:10.3415/VCOT-15-11-0184.
- Ashour AE, Hoffman CL, Muir P. 2019. Correlation between orthopaedic and radiographic examination findings and arthroscopic ligament fibre damage in dogs with cruciate ligament rupture. Aust Vet J. 97(12):490–498. doi:10.1111/avj.12878.
- Voss K, Karli P, Montavon PM, Geyer H. 2017. Association of mineralisations in the stifle joint of domestic cats with degenerative joint disease and cranial cruciate ligament pathology. J Feline Med Surg. 19(1):27–35. doi:10.1177/1098612X15606774.
- Frey TN, Hoelzler MG, Scavelli TD, Fulcher RP, Bastian RP. 2010. Risk factors for surgical site infection-inflammation in dogs undergoing surgery for rupture of the cranial cruciate ligament: 902 cases (2005-2006). J Am Vet Med Assoc. 236(1):88–94. doi:10.2460/javma.236.1.88.
- Motz AK, St Germaine LL, Hoffmann DE, Sung J. 2023. A retrospective evaluation of the effect of oclacitinib (Apoquel) administration on development of surgical site infection following clean orthopedic stifle surgery. PLoS ONE. 18(8):e0289827. doi:10.1371/journal.pone.0289827.
- Budsberg SC, Torres BT, Sandberg GS. 2021. Efficacy of postoperative antibiotic use after tibial plateau leveling osteotomy in dogs: A systematic review. Vet Surg. 50(4):729–739. doi:10.1111/vsu.13603.
- Sanders BD, McDonald-Lynch M, Kruse MA. 2024. Influence of antiseptic lavage during tibial plateau leveling osteotomies on surgical site infection in 1422 dogs. Vet Surg. 53(1):167–174. doi:10.1111/vsu.14050.