Whether it is the young puppy or kitten with an increased respiratory rate and effort or the patient that presents after trauma with respiratory difficulty, diaphragmatic hernias are not uncommon. Traumatic diaphragmatic hernias are more common than congenital, making up 85 percent of all such cases.1
Regardless of the cause, thorough patient evaluation and treatment of concurrent injuries is critical for successful outcome. Prompt diagnosis and appropriate perioperative management can lead to successful outcomes in the majority of cases.
Anatomy
The diaphragm is a musculotendinous structure that separates the abdominal and thoracic cavities. It is comprised of four muscle groups: pars lumbalis, pars sternalis, and paired pars costalis muscles, as well as a central tendon.
The attachment of the diaphragm includes ribs eight-13, lumbar vertebrae and sternum. From the abdominal view, the diaphragm is concave with attachments between the liver and stomach. Phrenic arteries provide blood supply to the diaphragm and innervation is provided by phrenic nerves. Three natural openings are present. including the aortic hiatus, esophageal hiatus, and the caval foramen.
Pathophysiology
Congenital hernias include pleuroperitoneal and peritoneopericarial hernias. The latter may be asymptomatic and 40 percent of cases are associated with another congenital defect.2 Hiatal hernias involve protrusion of viscera through the esophageal hiatus into the thorax. Traumatic diaphragmatic hernias are the most common form and account for 85 percent of all diaphragmatic hernias.1 Blunt force trauma (motor vehicle, falls, kicks) are the most common cause in veterinary patients. The costal muscles are the most likely component of the diaphragm to be involved. The remainder of this discussion will focus on traumatic hernias.
Diagnosis
When evaluating a patient following high-impact trauma, diaphragmatic hernia needs to remain on the list of possible differentials. On physical exam, patients may be dyspneic. Auscultation may identify muffled cardiac sounds and occasionally borborygmi. Occasionally, the abdomen may have an empty feeling on palpation. A thorough diagnostic workup for a trauma patient should include thoracic and abdominal radiographs. Abdominal viscera in the thoracic cavity is diagnostic for a diaphragmatic hernia. (Figures 1 and 2)

Treatment
Anesthesia considerations
With traumatic diaphragmatic hernias, the normal separation of the thoracic and abdominal cavities is lost. Assisted ventilation is critical in these patients. As soon as the incision is made on the ventral midline, the shared abdominal and thoracic cavity will be entered.
Timing of diaphragmatic hernia repair has been debated. Ninety-one percent of dogs that went to surgery within 24 hours of admission to the hospital, survived to discharge.3
A patient should be taken to the operating room for repair as soon as it is stable. If the patient is being treated for other life-threatening conditions, close monitoring is encouraged to look for decompensation.
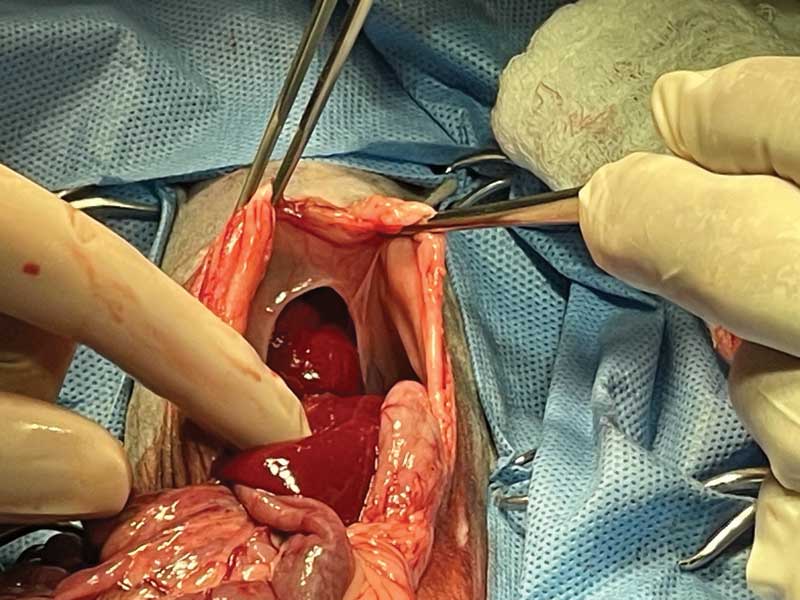
Surgical approach
A routine ventral midline incision is made, extending from the xyphoid to at least the umbilicus. The incision can be extended if needed for better visualization. The falciform fat can be excised to aid in visualization and easier closure of the linea alba. The cavity is exposed. Gentle traction can be used to return the abdominal contents to the correct position. Care is taken as the liver and spleen may be friable due to trauma. Thorough examination of all viscera is important to look for injuries such as liver laceration, liver lobe torsion, intestinal perforation, body wall trauma, etc.
Once the abdominal contents have been examined, the diaphragm and thoracic contents are evaluated. Slow re-inflation of the lungs is completed, and fluid is suctioned from the thorax.
To aid in visualization of the hernia, moistened laparotomy sponges can be used to protect the abdominal viscera. Balfour and malleable retractors are used to expose the diaphragm. The entire structure should be evaluated to determine the location and extent of the hernia, as well as ensure only one traumatic rent is present.
Primary closure of the hernia is completed with absorbable monofilament suture. A simple continuous pattern, starting at the dorsal most aspect of the hernia, is commonly used, although other patterns are appropriate.
Simple continuous patterns leave less potentially irritating suture material in the body. The initial suture tag may be left longer (temporarily) and used to apply tension to the repair site. Fresh diaphragmatic hernias can generally be repaired with a primary closure as there is a normal amount of tissue, and if treated efficiently, there should be minimal scar tissue and muscle contracture.
If the defect is more chronic, some of the wound edges can be freshened. Caution must be used to not remove too much tissue, which would prevent primary closure of the hernia. If the defect cannot be closed primarily, flaps using muscle or omenteum or polypropylene mesh can be used.
If the hernia involves a natural hiatus of the diaphragm, care must be taken to not close with enough tension to cause compression of the structures that naturally pass through the opening (vena cava esophagus, etc.). A thoracostomy tube is placed to allow removal of air and fluid in the early recovery period.
Once you have ensured no additional treatment is needed for any of the viscera, the abdomen is closed routinely. In chronic hernias, the abdominal wall may be difficult to close due to muscle contraction and/or lack of development in congenital hernias. A small malleable retractor placed in the incision and held by an assistant is useful in keeping the viscera protected in the abdomen while sutures are placed.
Postoperative care
Intravenous fluids and pain medications are appropriate until the patient can eat, drink, and take oral medications. Postoperative antibiotics are not generally needed. Frequent aspiration of the thoracostomy tube to remove residual air and fluids should be completed. The volumes obtained from the tubes are recorded to monitor for trends. When volumes decrease to 2-3 mL/kg/day, the tube may be removed.1
Complications
Increased intra-abdominal pressures can be seen in patients with repair of chronic hernias due to abdominal wall contraction or lack of development. Symptoms include hypoxia, decreased renal function, and discomfort. Although intra-abdominal pressures can be measured, it is not done routinely. Re-expansion pulmonary edema occurs in some cases and carries a guarded prognosis. Slow, controlled reinflation of the lungs is recommended to avoid this condition.
Outcome
While the majority of patients survive to discharge following a surgical correction of traumatic diaphragmatic hernias (80-85 percent),3,4 the complication rate may be as high as 50 percent.1
The first 24 hours after repair are the most critical for development of potentially life-threatening complications. These may include pulmonary edema, pneumothorax and hemothorax. Failure of the repair site is uncommon.
Successful management of diaphragmatic hernias is possible with efficient diagnosis, meticulous anesthetic management, and knowledge of relevant anatomy.
Kendra Freeman DVM, MS, DACVS, is a graduate of Colorado State University and maintains dual certification with the American College of Veterinary Surgeons. Dr. Freeman is an associate surgeon in Albuquerque, N.M. Her case load consists of orthopedics, general soft tissue, and sports medicine cases with the occasional return to her roots in large animal lameness and surgery.
References
- Tobias, Karen. Manual of small animal soft tissue surgery. John Wiley & Sons, 2017.
- Morgan, Keaton RS, et al. “Outcome after surgical and conservative treatments of canine peritoneopericardial diaphragmatic hernia: a multi‐institutional study of 128 dogs.” Veterinary Surgery 49.1 (2020): 138-145.
- Gibson, Thomas WG, Brigitte A. Brisson, and William Sears. “Perioperative survival rates after surgery for diaphragmatic hernia in dogs and cats: 92 cases (1990–2002).” Journal of the American Veterinary Medical Association 227.1 (2005): 105-109.
- Legallet, Claire, Kelley Thieman Mankin, and Laura E. Selmic. “Prognostic indicators for perioperative survival after diaphragmatic herniorrhaphy in cats and dogs: 96 cases (2001-2013).” BMC veterinary research 13.1 (2016): 1-7.