Last month, I addressed a case of a large mandibular tumor in a dog, which turned out to be a good prognosis of a benign peripheral odontogenic fibroma. This month, I am covering a similar case where a concerning swelling of the mandible turns out to have a good prognosis, but due to a different etiology.
Presentation
Cooper, a nine-year-old male shepherd mix, was presented for a right mandibular swelling. His owner first noticed the swelling approximately one month prior, and when she tried to look in Cooper’s mouth, the dog winced in pain. Cooper was eating normally, but may have been slightly more lethargic than usual. Bloodwork done at the time was unremarkable. Cooper’s primary care veterinarian recommended referral for assessment and possible biopsy.
On initial exam at our hospital, Cooper was bright and alert. Palpation of his temporal and masseter muscles showed significant atrophy bilaterally, which resulted in prominence of his zygomatic arches and sagittal crest. Mandibular lymph nodes palpated normally. There was a 4 cm x 3 cm x 2 cm mass arising from the lateral and ventral aspect of the right mandibular body (Figure 1 A). The mass was bony, rather than a fluctuant or soft tissue consistency.

the right ventral mandibular body (arrows). Photos courtesy Dr. John R. Lewis.
Cooper’s owner was concerned about the possibility of neoplasia based on her discussions with their primary care veterinarian. Bony neoplasia, such as osteosarcoma, had to be on the list of possibilities. However, there was some hope it could be something less insidious based on our conscious examination.
There were multiple fractured teeth dorsal to the swelling (Figure 1 B). These fractured teeth could be a source of endodontic disease. Perhaps the most encouraging bit of information we received from the owner was that the swelling did respond somewhat to antibiotics that were prescribed by her primary care veterinarian. The other encouraging aspect of the exam was there was no fleshy, proliferative soft tissue component to the swelling.

After discussion with Cooper‘s owner, we agreed thoracic radiographs would be a good idea prior to anesthesia to ensure there was no evidence of metastasis if the jaw mass was an osteosarcoma. Thoracic radiographs were interpreted by a board-certified radiologist and were found to be within normal limits.
Diagnosis
After receiving this information, we placed Cooper under general anesthesia. Anesthetized examination revealed a bony swelling that was centered ventral to the roots of tooth 408. Although none of the fractured teeth in the area of the swelling showed overt pulp exposure, dental radiographs revealed periapical lucencies of teeth 409, 408, and possibly 407. (Figure 2 A). This provided us with a possible cause/effect relationship. A radiograph of the ventral bony swelling showed a periosteal reaction in the absence of lysis, which was also interpreted as good news (Figure 2 B). Based on this evidence, we recommended extracting the fractured teeth and performing a biopsy of the bone in the area of the swelling.
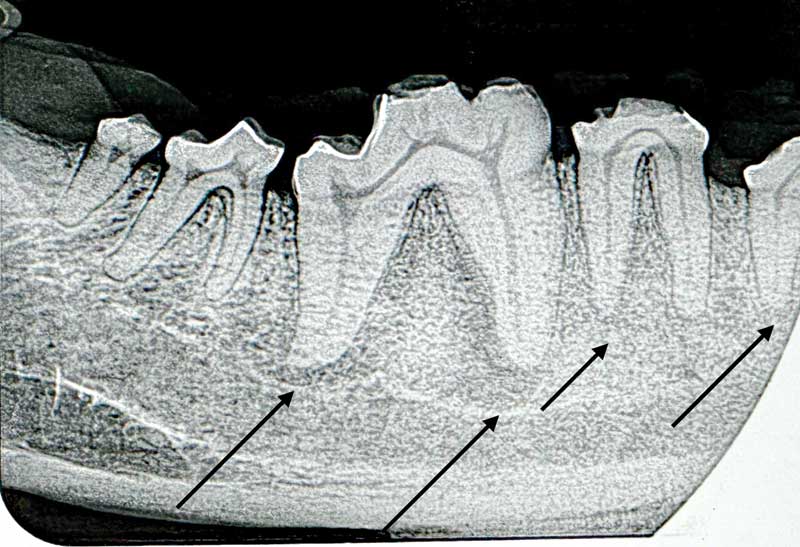
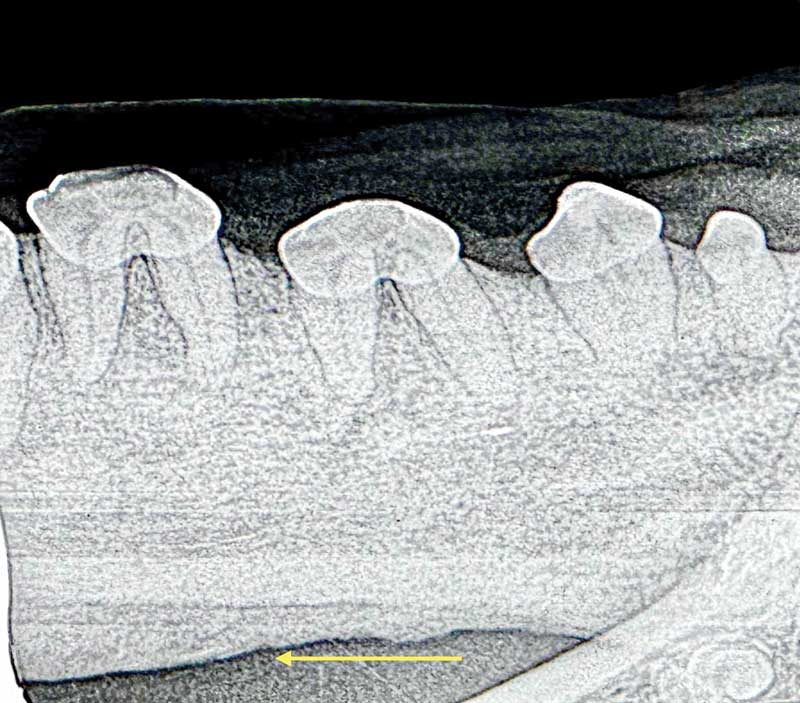
mandible (arrow).
Surgery
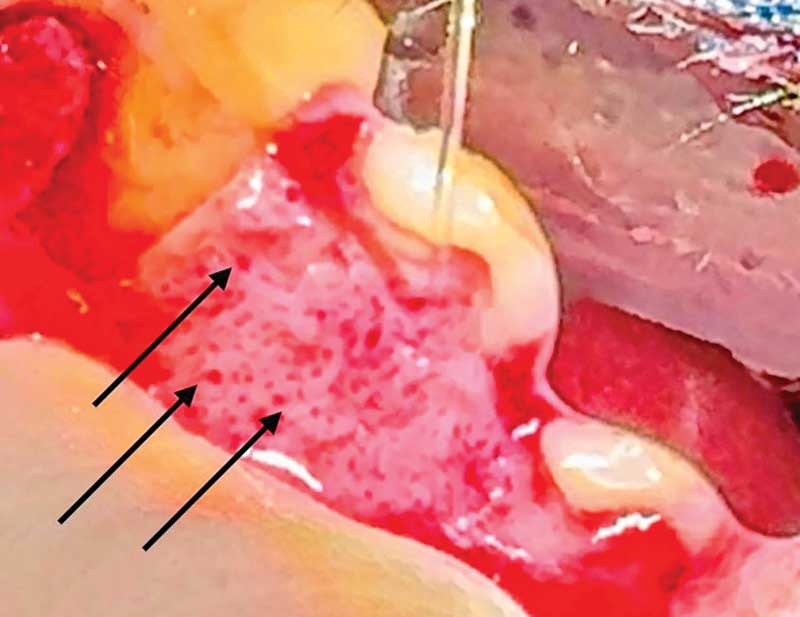
A mucoperiosteal flap was raised to remove teeth 407, 408 and 409. Multiple punctate areas of what appeared to be neovascularization were seen in the bone (Figure 3). A #2 round bur was used to create a window in the bone lateral to each root, and a 702 surgical bur was used to section the two-rooted teeth into separate crown-root segments.
After the teeth were removed, bone samples were obtained for aerobic/anaerobic bacterial culture and sensitivity and for histopathology. Culture showed no growth and histopathology of furcational bone showed no evidence of neoplasia, but rather reactive woven bone, edema, and fibrosis. These changes were suspected to be due to an adjacent osteomyelitis more ventrally.
The site was closed with 4-0 simple interrupted sutures of Poliglecaprone-25. Cooper was placed on a three-week supply of clindamycin at 10 mg/kg twice daily. At recheck, Cooper’s surgery site was healed, and he seemed more comfortable and less head shy.
Mandibular osteomyelitis occurs most commonly due to bacterial extension into the bone from endodontic infection or periodontal infection. Idiopathic osteomyelitis/osteonecrosis occurs in some dogs due to unknown reasons. Unlike Cooper’s case, osteonecrosis often results in formation of a sequestrum of bone that has completely lost its blood supply. In these cases, the sequestrum must be removed to have any chance of healing. Osteoradionecrosis can be seen in patients with a history of radiation therapy. Bisphosphonate-related osteonecrosis has been described in humans and our veterinary patients.
Cooper’s case was more straightforward: we removed the teeth that harbored the bacterial infection and placed him on postoperative antibiotics. Antibiotic choice can be guided by culture and sensitivity if growth is seen on the culture. Since anaerobes are difficult to grow, it is not uncommon that cultures may be negative. If so, clindamycin, amoxicillin/clavulanate or metronidazole are good empiric choices.
John R. Lewis, VMD, DAVDC Fellow, AVDC OMFS, practices at Veterinary Dentistry Specialists and teaches at Silo Academy Education Center, both in Chadds Ford, Pa.