
Photo courtesy Jessica McCarthy
Many of us who perform long days of surgery will be familiar with the aching neck or lower back as you sit on the sofa recuperating from the day. Occupational injury is common among veterinary surgeons, reported to be around 71 percent over a 10-year period, resulting in many missed workdays.1 Perhaps, unsurprisingly, the most common injuries are those caused by the patients themselves: bites and scratches. However, musculoskeletal injuries are also reported.1
Musculoskeletal injury in those performing surgery has been well studied in human medicine, but a small pilot study of veterinary surgeons showed a 17-degree angle of neck flexion and activation of the right trapezius muscle while performing surgery, with the highest rates of trapezius activation seen when doing orthopedic surgeries.2
To reduce the incidence of these injuries, it has been suggested to institute a preoperative checklist specific to the operating room set-up.3 Check listing is now commonplace in aerospace, human intensive care units, and in operating rooms. It reduces the errors that come when memory alone is relied upon. The World Health Organization (WHO) recommends the use of the Surgical Safety Checklist in all operative procedures.4
In addition, a group of trauma surgeons from Oxford University, England, recommend the use of the TULIPS mnemonic prior to every surgery to attain the optimum operating room setup.
T – Table position
U – You and your position
L – Lighting position
I – Imaging (such as intraoperative fluoroscopy) position
P – Patient and personnel position
S – Screen displaying any required images (radiographs) position
During the trial implementation period of TULIPS in the study, 93 percent of surgeons reconsidered, adjusted their surgical setup, and found the checklist helpful prior to surgical procedures.3
Table position
Table height should be set so that the operating surgeon’s forearm creates a 90-degree angle with their upper arm. The wrists should be able to be held in slight extension with a bend in the fingers.
You and your position
Avoiding forward head position (Figure 1) is important to reduce degenerative changes within the cervical spine.5 It is common for a surgeon’s shoulders to rise, particularly in stressful situations. Therefore, it is important to remember to relax the shoulders throughout the procedure. It is suggested to do periodic arm raises (while maintaining sterility) during longer procedures, particularly during laparoscopy, to encourage retraction of the scapula. If you are performing laparoscopy, ensure you are positioned to be able to maintain relaxed shoulders while keeping your forearms parallel to the floor, this may require the use of a stool (Figure 2).5
Feet should be kept hips width apart, with your weight evenly distributed to ensure pelvic girdle symmetry. The knees should not be locked out and deep muscles of the trunk and pelvis should be engaged to maintain a neutral posture. Postural resets can be performed by squatting intermittently, again. while maintaining the sterile field.5
Anti-fatigue mats may help reduce lower body fatigue, and compression socks, even at light pressure, have been shown to reduce lower leg fatigue and oedema.6
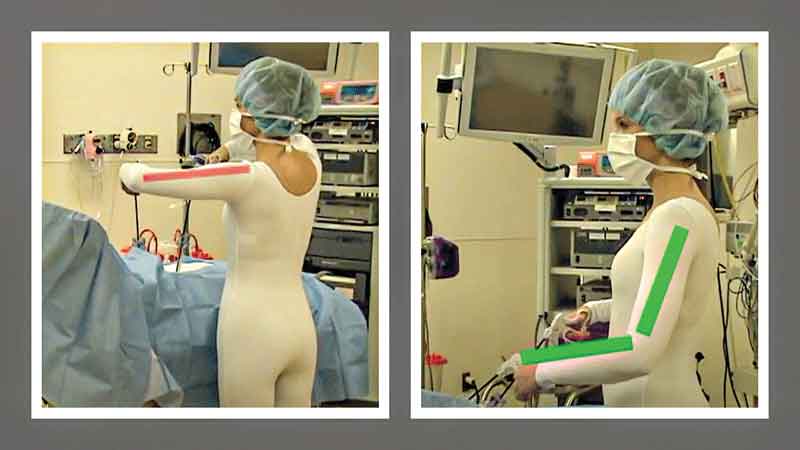
Photo courtesy PL Rosenblatt
Lighting position
Adjusting your lighting prior to scrubbing in is encouraged, as frequent handling of light can increase the risk of bacterial contamination.
Investing in good lighting will reduce risk to your patient and help maintain your own vision. If you are looking at screens, such as during a laparoscopy, dim the ambient light to prevent glare bouncing off the screens.
Imaging position
When using intraoperative fluoroscopy, it is imperative to check positioning prior to scrubbing in. It should be confirmed that the position of both the patient and the imaging unit are appropriate to allow imaging of the desired area. Consider what multiple views you may like to take intraoperatively.
Aim to reduce radiation exposure to surgeons and staff to As Low As Reasonably Achievable (ALARA), keeping in mind that orthopedic surgeons have a higher risk of cancer due to radiation exposure from C-arm fluoroscopy.7 Where possible, position the patient and C-arm where there is space for everyone to step away from the fluoroscopy system during its use.
Patient and personnel position critical
The positioning of the patient should provide comfort, avoiding pressure on bony prominences, such as the ilium or spine, particularly in larger breed dogs, where their body weight can result in injury from surgical positioning. Use appropriate padding and consider adding additional padding in larger patients. During laparoscopy for ovariectomy, for example, positioning and the ability to alter positions is important to allow visualization of the ovaries themselves.8
Check the surrounding area for wires or hazards personnel may encounter as they move around the patient during assisting. Communicate these hazards to avoid tripping or other injuries. Communicate with personnel where the sterile area begins and make sure the anesthetist has adequate access to their patient before the procedure starts.
Screen position
Screens should be positioned 10-25 degrees below the line of sight and directly ahead of the surgeon performing the procedure.9 This is not always possible, but consider the room layout with a goal of optimizing screen position and minimizing neck strain. It may be best to schedule laparoscopic procedures earlier in the day, when your neck is least fatigued. Remember to take regular postural breaks from turning your neck towards the screen and
employ a postoperative neck stretching routine.
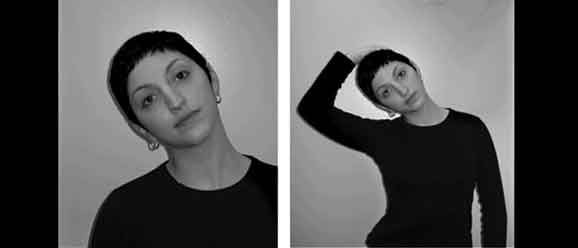
Photo courtesy Hullfish KL
Postoperatively
Despite our best intentions, many veterinarians can still have soreness and tightness after surgery. Make it part of your postsurgical routine to stretch your neck (Figure 3), hamstrings, and back as soon as you have changed out of your scrubs. Pilates, yoga, and regular massages have been recommended for surgeons to help reduce long-term discomfort.10 Products, such as strength training devices, claim to reduce neck pain and strain by strengthening the postural muscles. It is worth considering muscle strengthening as part of an anti-fatigue regime.11
As veterinarians, we are often notoriously bad at looking after ourselves, while giving everything to look after our patients. The TULIPS tool will allow you to take an extra couple of minutes of the day to consider yourself, as well as optimizing your surgical procedures and your ability to provide outstanding patient care.
Ask your nurses and assistants to remind you to take postural breaks, which will not only allow your body a moment of recovery, but also your mind. You will feel the difference when you get home at night, not only in your once-aching neck, but hopefully in the slightly lessened exhaustion you feel by allowing yourself more regular breaks in concentration throughout the day.
Jessica McCarthy, BVSc, MRCVS, DECVS, works as a faculty in orthopedic surgery at the University of Wisconsin. Dr. McCarthy became a diplomat of the European College of Veterinary Surgeons in 2020, after completing her residency training at the University of Edinburgh. McCarthy attended Bristol University for her veterinary degree and spent two years in general practice in England after graduating. She has a particular interest in elbow disease, both developmental and traumatic, and is passionate about ensuring everyone in the veterinary profession can work in a diverse and inclusive atmosphere.
Faolain Barrett, BVM&S, is a surgery resident at the University of Wisconsin. Dr. Barrett has a love for feline orthopedics and has performed research on how veterinary surgeons can improve the classification of intraoperative and postoperative complications.
References
- Jeyaretnam J, Jones H, Phillips M. Disease and injury among veterinarians. Aust Vet J. 2000 Sep;78(9):625–9. https://pubmed.ncbi.nlm.nih.gov/11022291/
- Asadi H, Simons MC, Breur GJ, Yu D. Characterizing Exposure to Physical Risk Factors during Veterinary Surgery with Wearable Sensors: A Pilot Study. IISE Transactions on Occupational Ergonomics and Human Factors. 2022 Sep 14;10(3):151–60. https://pubmed.ncbi.nlm.nih.gov/36008924/
- Neal-Smith G, Kim DS, Wood A. A Review of Orthopaedic Surgical Set-Up and Introduction of the TULIPS Mnemonic – Six Simple Steps for Optimising Set-Up in Orthopaedic Surgery. Cureus. 2020 Aug 17; https://pubmed.ncbi.nlm.nih.gov/32953318/
- Tool and Resources [Internet]. [cited 2023 May 2]. Available from: https://www.who.int/teams/integrated-health-services/patient-safety/research/safe-surgery/tool-and-resources
- Rosenblatt PL, McKinney J, Adams SR. Ergonomics in the operating room: protecting the surgeon. J Minim Invasive Gynecol. 2013 Aug 20;20(6):744. https://pubmed.ncbi.nlm.nih.gov/23969139
- Garcia M-G, Roman MG, Davila A, Martin BJ. Comparison of physiological effects induced by two compression stockings and regular socks during prolonged standing work. Hum Factors. 2021 Jun 2;187208211022126. https://pubmed.ncbi.nlm.nih.gov/34078143/
- Mastrangelo G, Fedeli U, Fadda E, Giovanazzi A, Scoizzato L, Saia B. Increased cancer risk among surgeons in an orthopaedic hospital. Occup Med (Lond). 2005 Sep;55(6):498–500. https://pubmed.ncbi.nlm.nih.gov/16140840/
- Liehmann LM, Seny T, Dupré G. Effect of patient rotation on ovary observation during laparoscopic ovariectomy in dogs. Vet Surg. 2018 Jun;47(S1):O39–51. https://onlinelibrary.wiley.com/doi/abs/10.1111/vsu.12764
- Menozzi M, von Buol A, Krueger H, Miège C. Direction of gaze and comfort: discovering the relation for the ergonomic optimization of visual tasks. Ophthalmic Physiol Opt. 1994 Oct;14(4):393–9. https://pubmed.ncbi.nlm.nih.gov/7845698/
- Hullfish KL, Trowbridge ER, Bodine G. Ergonomics and gynecologic surgery. Journal of Pelvic Medicine and Surgery. 2009 Nov;15(6):435–9. https://www.researchgate.net/publication/238156373_Ergonomics_and_Gynecologic_Surgery
- Iron Neck Training | Neck Exercise Machine & Strengthening Equipment [Internet]. [cited 2023 May 2]. Available from: https://www.iron-neck.com/?gadid=&utm_source=google&utm_medium=paid&utm_campaign=17217398873&utm_content=&utm_term=&hsa_acc=6538825685&hsa_cam=17217398873&hsa_grp=&hsa_ad=&hsa_src=x&hsa_tgt=&hsa_kw=&hsa_mt=&hsa_net=adwords&hsa_ver=3&gclid=Cj0KCQjw6cKiBhD5ARIsAKXUdyaP99tQFVclKdFVoniXjKXBhN09MIf37ysGrpvyVXkUV_u4gtAxj_waAoA9EALw_wcB