 Dental disease in rabbits and herbivorous rodents (mainly guinea pigs, chinchillas, and degus) typically involves overgrowth of the clinical crowns, development of intraoral dental points, and/or overgrowth of the apices of the teeth (mandibular teeth, maxillary teeth, or both). There are many proposed etiologies of dental disease in these species, which likely means it is a multi-factorial process.
Dental disease in rabbits and herbivorous rodents (mainly guinea pigs, chinchillas, and degus) typically involves overgrowth of the clinical crowns, development of intraoral dental points, and/or overgrowth of the apices of the teeth (mandibular teeth, maxillary teeth, or both). There are many proposed etiologies of dental disease in these species, which likely means it is a multi-factorial process.
Treatment of dental disease in rabbits and herbivorous rodents commonly requires repeated dental trimming, often for the remainder of the patient’s life. Additional complications, such as dental abscessation, are common in certain species.
Rabbits
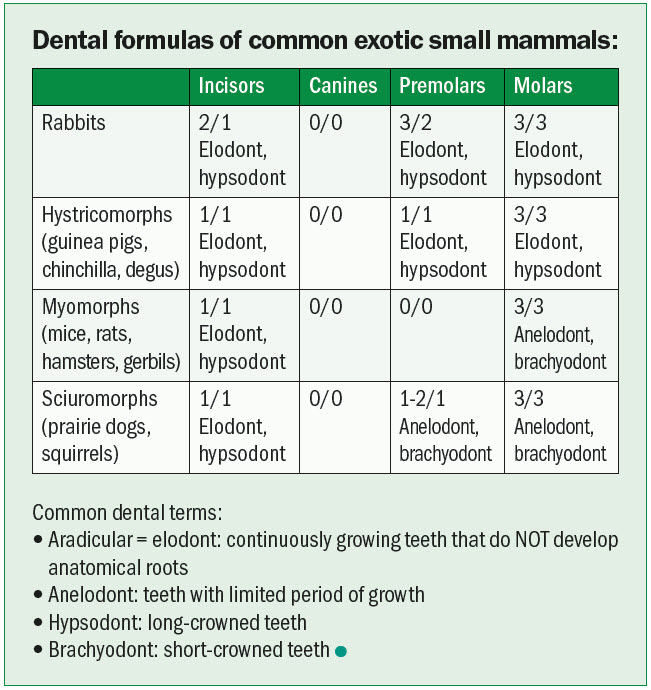
All rabbit teeth are hypsodont (high-crowned) and open-rooted (elodont), which means they grow continuously throughout life and never develop anatomic roots. Their teeth are composed of a clinical crown (visible above the gingiva), reserve crown (sub-gingival), and apex. None of their teeth have anatomic tooth roots (Figure 1A); therefore, the term “tooth-root abscess” is not appropriate with rabbits. The first maxillary incisors and mandibular incisors of rabbits grow approximately 2 to 3 mm per week (Figure 1B).

Rabbits are anisognathic—their maxilla is wider than the mandible. Their chewing motions vary for each type of substrate they ingest. When chewing natural vegetation (hay, greens, grasses), the major chewing motion (“power stroke”) is horizontal. This leads to a normal wearing pattern of all the teeth. When rabbits eat a pelleted diet or grains, the major chewing motion is more vertical, which leads to uneven tooth wear over time.
Rabbits have a ~10 degree angle of occlusion for their premolars and molars. This is important to maintain, if possible, with occlusal adjustments (dental trims). Their incisors have a chiseled edge due to reduced enamel on the lingual compared with the facial surface—this angle should be maintained when performing dental procedures.

Etiology
There are several proposed causes for dental disease in rabbits, and it is likely a multifactorial disease. Some of the more common hypotheses include genetics (dwarf breeds more predisposed), metabolic bone disease, inappropriate diet (lack of hay and other abrasive dietary items), trauma, and aging.
Dental disease in rabbits is often chronic and progressive, which has been described in three continuous and sometimes overlapping stages: early changes, acquired malocclusion, and late changes.
The early changes include apical elongation of the teeth and enamel hypoplasia. Elongated mandibular premolars and molars can be palpated on the ventral aspect of the mandibles, and elongated maxillary premolars and molars can sometimes be palpated ventral to the eyes. This can be painful, and owners may notice the rabbit refusing to eat harder foods, such as hay. Epiphora may also be noted due to partial or complete occlusion of the nasolacrimal duct by apical elongation of the maxillary incisors and/or premolars.
Acquired malocclusion is the next stage, and is characterized by development of dental points or spurs from inappropriate wear on the premolars-molars.
The final stages involve fractured crowns, and uneven teeth due to destruction of the germinal tissue which will lead to cessation of growth. Common complications of chronic dental disease include apical tooth abscesses and dacryocystitis (chronic infection of obstructed tear ducts).
Oral exam and diagnostics
A limited oral exam can be performed on awake patients, with either an otoscope cone or a human nasal speculum (my preference). The view of the caudal-most teeth is limited, and a complete oral exam often requires heavy sedation or general anesthesia.
Due to the natural chewing motions of rabbits, dental points will most likely be found on the lingual surface of the mandibular premolars/molars and the buccal surface of the maxillary premolars/molars. Any purulent material or foul odor in the mouth should be noted.
The clinician should also thoroughly palpate the ventral surface of each mandible and ventral to each eye for any masses or asymmetry. Ideally, some form of imaging would be obtained from each patient with suspected dental disease to help determine the extent of the sub-gingival disease.
Computed tomography is superior to skull radiographs for imaging of the soft tissues of the skull; however, this is not always possible for every patient. Heavy sedation or brief anesthesia is required for proper positioning for skull radiographs, and a complete series includes a straight lateral (with both bullae superimposed), right lateral oblique, left lateral oblique, and a ventrodorsal (or dorsoventral) view.
Treatments
Numerous treatment methods for dental disease in rabbits have been published. Before treatment is initiated, no matter which methodology, the owner should be notified dental disease in rabbits often requires life-long treatment, and a single procedure is not likely to be curative.
Occlusal adjustments should be performed on anesthetized rabbits—ideally, they would also be intubated and have IV access. A round-tipped bur or similar-sized bur on a slow-speed handpiece for premolar and molar adjustments (Figure 2), and the high-speed handpiece with a variety of burs for incisor adjustments. The clinician should attempt to correct the dental abnormalities, so they approximate, as closely as possible, the normal occlusion rather than reducing the clinical crowns as short as possible.

Several treatments for dental-related abscesses in rabbits have been published, including marsupialization, complete abscess excision, and packing the abscess with a variety of antibiotic impregnated items (PMMA beads, gauze, umbilical tape, etc.).1,3,12
With the marsupialization technique, a large punch biopsy is used to create a hole in the skin and abscess capsule. The abscess is debrided and flushed with dilute chlorhexidine and saline, and the skin edges sutured to the edge of the abscess capsule with simple interrupted sutures. The abscess capsule is flushed, ideally, twice daily at home with the owner, and the skin defect usually heals closed within five to seven days. As rabbit pus is not liquid, it will not drain like a cat/dog abscess. Therefore, lancing and drain placement is inappropriate and often ineffective for this species.
A recent retrospective study3 described a more extensive surgical excision of rabbit facial abscesses with good success. Extraoral tooth extractions for treatment of facial/dental abscesses has also been described in a recent case series;4 however, both this and extensive surgical excision techniques are more technically challenging and often require advanced imaging for surgical planning and post-operative monitoring.
Long-term antibiotics are often indicated in rabbits with dental disease, and especially those with apical abscesses. Treatment of abscess with antibiotics alone may reduce the size of the abscess during treatment, but it is unlikely to lead to complete resolution of the infection.
In a retrospective review of cultures of rabbit abscesses,6 100 percent of the strains tested were susceptible clindamycin (cannot safely be given orally to rabbits), 96 percent were susceptible to penicillin (can be given parentally to rabbits), 54 percent were susceptible to ciprofloxacin (enrofloxacin), and only seven percent were susceptible to trimethoprim-sulfamethoxazole.
A more recent study11 evaluated the microbiology and antibiotic susceptibilities of odontogenic abscesses in rabbits via retrospective analysis of rabbits that presented to the University of California (UC) Davis companion avian and exotics service over the last 14 years. The two most common anaerobic isolates were Fusobacterium spp. and Peptostreptococcus spp., and the most common aerobic isolates were Pseudomonas aeruginosa and Pasteurella sp. The large number of anaerobic bacteria cultured was unexpected, and possible safe options for anaerobic treatment in rabbits include penicillin (parenterally), chloramphenicol, and metronidazole.
Hystricomorph rodents (Guinea pigs and chinchillas)
Guinea pigs and chinchillas are the most common rodent species presented for dental disease. Chinchillas have a zero to 10-degree angle to their occlusal plane, versus guinea pigs that have a 30-degree angle. The growth rate of chinchilla premolars and molars is approximately three to four mm/month.
Guinea pig incisors grow at a rate like rabbits. In addition, their mandibular incisors are three times longer than the maxillary incisors, and this should not be misinterpreted as overgrowth. Guinea pigs and Russian hamsters lack ferric oxide (which looks yellow) in their enamel contrary to other rodent species (chinchillas).
Guinea pigs commonly have incisor malocclusion and mandibular (rather than maxillary) premolar-molar clinical crown overgrowth. Due to the angle of occlusion of their premolars and molars, bilateral clinical crown elongation of the guinea pig mandibular premolars can completely encase the rostral aspect of the tongue, also called tongue entrapment (Figure 3). This condition prevents the animal from properly prehending and swallowing food due to limited tongue movements, which can become a life-threatening condition if not treated promptly. Eighty percent of guinea pigs with dental disease have a low body condition score (BCS).14 Macrodontia (tooth enlargement) has also been reported in 89 percent of guinea pigs with dental disease according to a recent study, and the mandibular incisors were the most commonly affected teeth.13 Food impaction and gingivitis is significantly more common in chinchillas than guinea pigs and rabbits. Drooling and perioral staining are common clinical signs in chinchillas with dental disease, but are uncommonly seen in guinea pigs.

Diagnostics and treatments for rodents with dental disease are similar to those for rabbits, as described above. One study describes the use of computed tomography (CT) for the assessment of dental disease in 66 guinea pigs. Ninety-five percent of the guinea pigs in that study had a history of dysphagia, but only two of the guinea pigs showed ptylism.14 Other common presenting complaints of guinea pigs with dental disease were reduced body condition score (50 percent of patients) and diarrhea (30 percent). Obliquely worn incisors (Figure 4) were a common physical exam finding when there was incisor and premolar-molar malocclusion; dental fractures were noted in ~25 percent of all guinea pigs in the study.14 Overall, rodents have a significantly lower prevalence of dental disease compared to rabbits, and they are less prone to periapical abscesses and osteomyelitis.

Conclusion
All the teeth (incisors, premolars, and molars) in rabbits and hystricomorph rodents (guinea pigs and chinchillas) continuously grow; therefore, dental disease is a common in these species. The term “tooth-root abscess” is not accurate (or physically possible) as none of their teeth have anatomic roots. Clinical crown overgrowth, apical overgrowth, or both, can occur as a result of inappropriate tooth growth. Treatment typically involves reduction of crown height with a dental bur (slow-speed for the premolars and molars, and high-speed for the incisors).
Dental disease in these species is typically chronic and progressive, and repeated dental procedures are often needed for the remainder of the patient’s life. Additional complications of dental disease in these species (rabbits particularly) include dental apical abscesses and dacryocystitis.
Olivia A. Petritz, DVM, DACZM, graduated from Purdue University, and then completed several internships and a residency in the field of zoo and exotic animal medicine. Dr. Petritz became a diplomate in the American College of Zoological Medicine in 2013 and specializes in zoological companion animals (exotic pets). Petritz started an exotics service at a specialty hospital in Los Angeles following her residency, and currently is an assistant professor of avian and exotic animal medicine at North Carolina State University.
References
- Levy, Ivana, and Christoph Mans. “Long-term systemic antibiotics and surgical treatment can be an effective treatment option for retrobulbar abscesses in rabbits (Oryctolagus cuniculus): 21 cases (2011–2022).” Journal of the American Veterinary Medical Association 1.aop (2023): 1-7.
- Johnson, Jade C., and Charlotte C. Burn. “Lop‐eared rabbits have more aural and dental problems than erect‐eared rabbits: a rescue population study.” Veterinary Record 185.24 (2019): 758-758.
- Jekl, Vladimir, Edita Jeklova, and Karel Hauptman. “Radical debridement guided by advanced imaging and frequent monitoring is an effective approach for the treatment of odontogenic abscesses and jaw osteomyelitis in rabbits: a review of 200 cases (2018–2023).” Journal of the American Veterinary Medical Association 1.aop (2023): 1-10.
- Girard, Nicolas. “Surgical Treatment of Facial Abscesses and Jaw Osteomyelitis of Dental Origin Using Extraoral Tooth Extraction in the Domestic Rabbit: A Case Series.” Journal of Veterinary Dentistry (2023): 08987564231168985.
- Artiles, Charles A., et al. “Computed tomographic findings of dental disease in domestic rabbits (Oryctolagus cuniculus): 100 cases (2009–2017).” Journal of the American Veterinary Medical Association 257.3 (2020): 313-327.
- Tyrrell KL, Citron DM, Jenkins JR, Goldstein EJC, Group VS. Periodontal Bacteria in Rabbit Mandibular and Maxillary Abscesses. Journal of Clinical Microbiology. March 1, 2002 2002;40(3):1044-1047.
- Boehmer E, Crossley D. Objective interpretation of dental disease in rabbits, guinea pigs and chinchillas. Tierrztliche Praxis Kleintiere. 2009;4:250-260.
- Legendre LÃF. Oral disorders of exotic rodents. Veterinary Clinics of North America: Exotic Animal Practice. 2003;6(3):601-628.
- Crossley DA. Oral biology and disorders of lagomorphs. Veterinary Clinics of North America: Exotic Animal Practice. 2003;6(3):629-659.
- Jekl V, Redrobe S. Rabbit dental disease and calcium metabolism: the science behind divided opinions. Journal of Small Animal Practice. 2013;54(9):481-490.
- Gardhouse, Sara, et al. “Bacterial isolates and antimicrobial susceptibilities from odontogenic abscesses in rabbits: 48 cases.” Veterinary Record (2017): vetrec-2016.
- Taylor, W. Michael, et al. “Long-term outcome of treatment of dental abscesses with a wound-packing technique in pet rabbits: 13 cases (1998–2007).” Journal of the American Veterinary Medical Association 237.12 (2010): 1444-1449.
- Köstlinger, Saskia, Sandra Witt, and Michael Fehr. “Macrodontia in guinea pigs (Cavia porcellus)–Radiological findings and localization in 131 patients.” Journal of Exotic Pet Medicine 39 (2021): 68-75.
- Schweda, M. C., et al. “The role of computed tomography in the assessment of dental disease in 66 guinea pigs.” Veterinary Record 175.21 (2014): 538-538.