By Anne S. Hale, DVM • VetStem, Inc.
As we adjust our practices to accommodate a focus on providing for all ages and stages of our patient’s lives, many veterinarians have been including cellular therapy to promote healing and pain control without a polypharmacy approach. There are several cellular therapies on the market with various claims relating to osteoarthritis control, wound healing, and pain control. Platelet-rich plasma (PRP) is one such biologic that has been utilized for decades to promote healing in acute and chronic soft tissue injuries, joint disease, corneal ulcers, chronic wounds, and more. Both large and small animals have benefitted from the presence of platelets during the healing process.
The Healing Properties of Platelet-Rich Plasma
Platelet-rich plasma is one of the most common biologics used in intra-articular, intralesional, and topical administration to assist with wound healing as well as inflammation and pain control. The goal is to deliver a concentrated dose of platelets to accelerate lagging internal healing processes by amplifying the biological signals that would naturally occur when platelets aggregate at a site of injury. In vitro and ex vivo testing of platelets as a part of the “cell healing team” suggests that PRP works due to the presence of platelet membrane interaction with damaged endothelium. This interaction leads to the expulsion of platelet alpha granules which are “packets” of growth factors and anti-inflammatory cytokines. These growth factors and cytokines signal to mesenchymal stem cells, macrophages, and T cells, which coordinate the healing process in the immediate region. Platelet alpha granules routinely0100 carry platelet-derived growth factor (PDGF-BB), vascular endothelial growth factor (VEGF), and CXCL12 (potent stem cell recruiter). In all, over 200 proteins have been identified in the granules that are associated with angiogenesis, wound healing, coagulation, and endothelial repair.
Platelets are anuclear organelles that have a limited lifespan of usually not more than 1-3 days when activated. When used as a biologic, PRP should have a suitable amount of alpha granule content available for action in that period of time. This translates to total platelet dose. Higher concentrations of platelets (>3X baseline) are recommended for intralesional and intra-articular treatment protocols based on published clinical trials. In the review of thirty papers published in the last ten years, a dosing structure of 3 to 8 times baseline has been associated with positive outcomes after administration of PRP.1,2
Platelet-Rich Plasma Production
Commonly, autologous PRP is produced from the patient’s whole blood using a mechanical device (kit) involving centrifugation to separate platelets and white cells from the rest of the whole blood. Typically, the mechanical device uses a proprietary tube often paired with a filtering gel or mechanism to segregate the platelets and plasma from whole blood. The purpose of these devices is directed towards platelet collection and concentration along with plasma. Leucocytes may or may not be included in the collection process depending on which system is used. Ideally, PRP should have minimal hemoglobin and red blood cell contamination as this can cause transfusion-like adverse events and antibody formation. Autologous PRP devices do not require FDA index or review before marketing.
Variability in Platelet-Rich Plasma Products
Autologous PRP has the advantage of minimizing the potential for transfusion reaction on administration of the product because the recipient donates their own blood for processing. However, autologous PRP production has several disadvantages that can impact the outcome in your patient’s response to therapy. Most commonly, autologous PRP production is negatively influenced by the inflammatory state of the patient, platelet count of the patient, operator handling of the sample, and the effectiveness of the PRP mechanism (kit) used to produce the product. This variability of the injectable product can lead to inconsistent or ineffectual treatment.
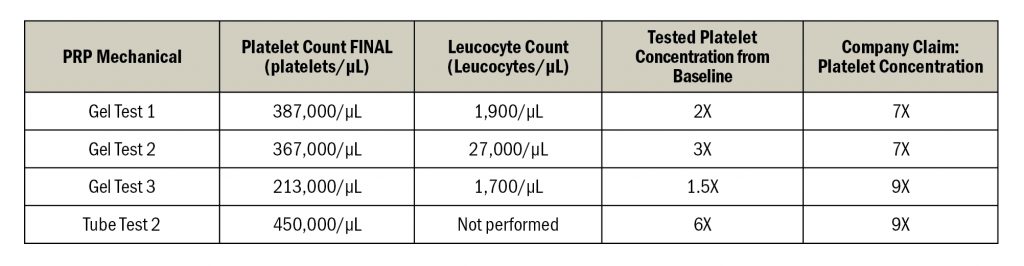
In a recent comparison of four PRP kits for the production of equine PRP, these kits demonstrated a lack of uniformity relating to the final platelet count and platelet concentration (Table 1). Variability was noted despite utilizing the same operator, centrifuge, and platelet counter. Outcomes, as indicated by platelet count in the PRP, were also variable. Additionally, each kit failed to meet their respective platelet concentration claim.
Allogeneic “Off-The-Shelf” Platelet-Rich Plasma
Platelet count directly correlates to the amount of growth factors and anti-inflammatory cytokines available for treating the joint, soft tissue lesion, or surface wound. Variability in therapeutic outcomes can occur when the product is not uniform, especially relating to platelet concentration and total platelet dose. The results above show wide variation between actual platelet concentration and that claimed by the PRP mechanical device manufacturer.
Newer generation allogeneic products like PrecisePRP avoid this variation by pooling donors and confirming the characteristics of the PRP during manufacture. This uniformity leads to a more consistent
avoid this variation by pooling donors and confirming the characteristics of the PRP during manufacture. This uniformity leads to a more consistent
patient response to the cellular therapy and is advantageous in older or more diseased patients whose autologous PRP production is negatively influenced by the inflammatory state of the patient.
Conclusion
PRP represents an affordable cellular therapy to offer your patient as an aid to healing through cell signaling to regenerative cells, control of inflammation, and the promotion of cell growth. A consistent and repeatable product, like any pharmaceutical, is key to the best patient outcomes.
References
- Garbin LC, et al. (2021), A Critical Overview of the Use of Platelet-Rich Plasma in Equine Medicine Over the Last Decade. Front. Vet. Sci. 8:641818.
- Everts P, et al., Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int J Mol Sci. 2020 Oct 21;21(20):7794.