Photos courtesy Kendra Freeman
Orthopedic injuries in our juvenile patients can be challenging and rewarding all at the same time. Puppies and kittens are resilient on so many levels. Their energetic and explosive antics can sometimes lead to injury, however, seemingly minor trauma can lead to serious injury.
A challenge with juvenile patients is deciding which injuries can be managed successfully without surgical intervention, and which ones will heal without surgery. Their rapid growth and excellent healing capacity allows for efficient healing, remodeling, and adaptation.
Although these young patients have exceptional capacity to heal, surgical intervention is sometimes indicated so that they may lead full, active lives, with minimal discomfort. Treatment should be focused on early return to function and mobility–which sometimes means “less is more” in the operating room for successful treatment.
Healing capacity
Juveniles have an excellent healing capacity, especially in their bones. Patients less than five months of age have relatively elastic bones with a thick covering of periosteum. This allows the immature bone to withstand larger forces before fracture. Once the bone fractures, callus formation is rapid and efficient due to an excellent blood supply.
Young patients may heal in as little as two to four weeks. This means it is critical to understand when to intervene surgically, and when to manage these cases conservatively. Growth plate and/or joint involvement are often criteria for surgical stabilization.
Juvenile fractures
Young animals are susceptible to some of the same long bone fractures as adults. Treatment should be focused on rapid return to function–pain management, realignment of the bone, and limited external coaptation.
Juvenile patients are susceptible to additional injuries not seen in mature animals. For example, green stick fractures are unique to young patients. These happen when the diaphysis of a long bone bends and cracks without breaking into separate pieces. With appropriate activity restriction and possibly a short-term bandage, these fractures can heal without surgical intervention. A proliferative callus may develop; however, this will remodel as the patient grows and bears weight on the limb.
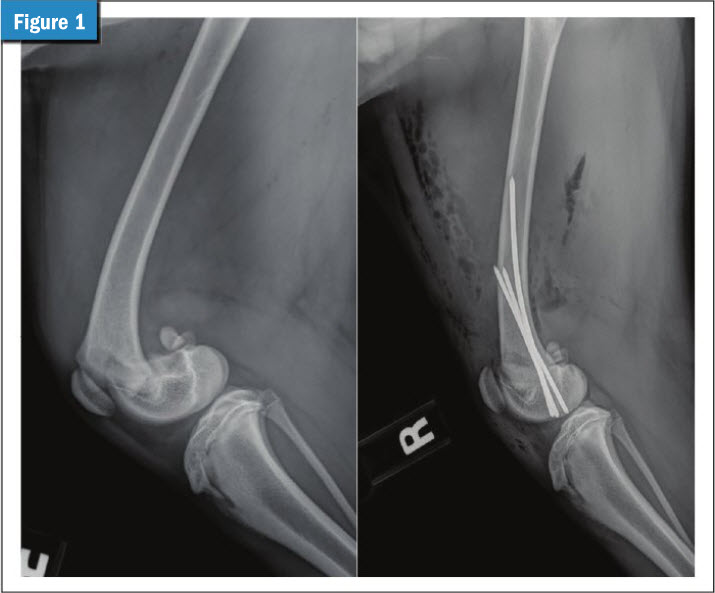
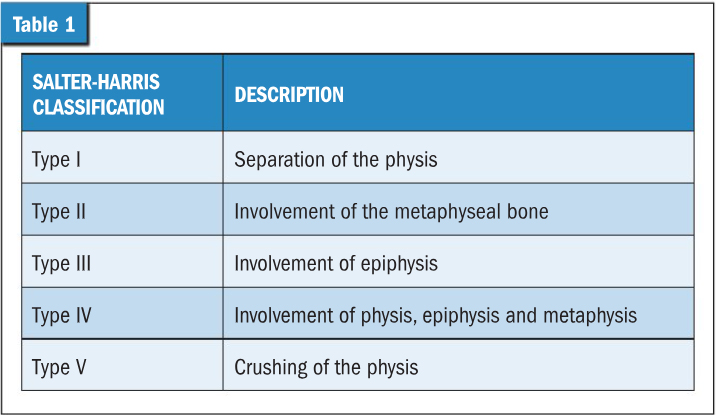
Since the physis (growth plate) and apophysis (bone outgrowth or tuberosity) in immature patients are often the path of least resistance, these structures are commonly injured, sometimes from seemingly minor events. The Salter-Harris classification system is used to describe the various types of growth plate injuries. Five different types have been identified, with Salter-Harris Type II being the most common (Table 1).1
Timing of treatment is critical in these cases. Young animals will try to heal these fractures quickly, although displaced fractures will not have appropriate alignment for healing. These displaced fractures should be stabilized within one week of the injury to allow for appropriate reduction and alignment and lesson the formation of perifracture fibrous tissue. The following are specific examples of juvenile fractures:
- Salter-Harris Type II fracture of the distal femoral physis (Figure 1). This fracture accounts for 60 percent of all femur fractures and is the most common physeal fracture in dogs.2 These fractures have caudal displacement of the distal fragment and require reduction and stabilization for a successful outcome. Delay in surgery will make reduction of the fracture difficult due to muscle contracture and proliferative fibrosis. These fractures can be stabilized with two to three intramedullary pins. With prompt and appropriate stabilization, these patients can have good to excellent outcomes.2
- Premature closure of the distal ulnar physis (Figure 2). The conical shape of the distal ulnar physis predisposes this site to a Salter-Harris Type V (crushing) injury. Indeed, 100 percent of ulnar length distal to the elbow joint happens from this growth plate, making this injury problematic in young growing animals.2 This injury can be challenging to diagnose immediately after the trauma.

With this injury only swelling may be present initially. The growth plate is not displaced, so radiographs shortly after the suspected trauma may be unrewarding. This injury only occurs in patients that have residual growth potential. As the radius continues to grow while the ulna does not, the limb often develops dorsal bowing, carpal valgus and humeroulnar incongruity.
In skeletally immature animals with residual growth potential, proximal ulnar osteotomy can be performed to allow the radius continued growth and improved alignment of the elbow joint as the patient matures.
Once the patient is skeletally mature a corrective osteotomy of the radius and osteotomy of the ulna is generally needed to improve alignment of the limb.
- Tibia tuberosity avulsion (Figure 3). This injury involves detachment of the apophysis (tuberosity) due to a pull from the patellar ligament. Due to the constant tug of the quadriceps mechanism, these fractures are often displaced. The presence of multiple growth plates in this region can sometimes make this diagnosis challenging, especially if the fragment is not displaced. A lateral radiographic projection of the opposite limb can be very helpful in identifying this injury. A concurrent Salter-Harris type II injury to the proximal tibia physis is not uncommon, and this physis should be evaluated closely on radiographs. Again, a similar projection of the contralateral limb is useful for comparison. If an injury is present in the proximal physis, the epiphysis is often caudally displaced.

Stabilization of this avulsion injury involves placement of Kirschner wires or Steinman pins and sometimes a wire placed in a figure eight pattern. This wire acts as a tension band to counteract the forces of the quadriceps mechanism. Traditionally, removal of the implants was recommended once the fracture has healed (four to six weeks after surgery) to limit continued disturbance of the growth of the bone. A recent study challenges this practice—when the metal implants were left in place, 93 percent of clients were satisfied and there was no difference in long term outcome.3
- Condylar fractures (Figure 4). The distal humerus epiphysis develops from two ossification centers. Fractures in this region involve the joint surface and are often Salter-Harris type III or IV fractures. These fractures account for about 40 percent of all humeral fractures,2 with French Bulldogs having the greatest risk for this injury.4 Since the joint is involved, urgent and meticulous joint re-alignment and stabilization of the fracture is needed for a successful outcome. Non-surgical management or long term immobilization is inappropriate for most of these patients. Even patients with timely, appropriate stabilization of the fracture remain at increased risk of development of osteoarthritis in the future.

Conclusion
Juvenile fractures are common and often require prompt treatment for a successful outcome. Thankfully, these patients heal quickly when timely treatment focuses on early mobility and return to function. So, the next time you are presented with a puppy or kitten that is lame after a seemingly minor event, radiographs are encouraged to rule out a potential issue, such as growth plate or joint injury that needs urgent, specific treatment.
Kendra Freeman DVM, MS, DACVS, is a graduate of Colorado State University and maintains dual certification with the American College of Veterinary Surgeons. Dr. Freeman is an associate surgeon in Albuquerque, N.M. Her case load consists of orthopedics, general soft tissue, and sports medicine cases with the occasional return to her roots in large animal lameness and surgery.
References
- DeCamp, Charles E., et al. “Flo’s Handbook of Small Animal Orthopedics and Fracture Repair.” Missouri: Elsevier 2016.
- Johnston, Spencer A., and Karen M. Tobias. Veterinary surgery: small animal expert consult. Elsevier Health Sciences. 2017.
- Miller, Zachary A., et al. “Good clinical outcomes achieved in young dogs with tibial tuberosity avulsion fracture repairs when implants were left in situ past skeletal maturity.” Journal of the American Veterinary Medical Association 022: 1-6. https://pubmed.ncbi.nlm.nih.gov/36170215/
- Sanchez Villamil, Carlos, et al. “Impact of breed on canine humeral condylar fracture configuration, surgical management, and outcome.” Veterinary Surgery 49.4.2020. 639-647. https://onlinelibrary.wiley.com/doi/full/10.1111/vsu.13432