A cat presenting in acute respiratory distress is not an uncommon occurrence in a veterinary emergency setting. However, a week with three black cats presenting similarly is notable. Emergencies such as the cat cases in this feature underscore the need for, and importance of, readily available in-house diagnostics (point-of-care) testing as an option for veterinary teams. In-time laboratory and imaging results in each of the following cases helped provide essential diagnostic information, allowing for timely and appropriate case management.
Case 1) Alby’s Pyothorax
Alby, a two-year-old male domestic shorthair cat, presented as an emergency due to his acute onset of respiratory distress, after progressive lethargy and anorexia. He was an indoor/outdoor cat with no previous history of health concerns or trauma.
Radiographs identified pleural effusion and therapeutic thoracocentesis was quickly performed. A portion of the opaque fluid collected was placed in an ethylenediaminetetraacetic acid (EDTA)-anticoagulated blood tube (Figure 1) for analysis, as well as a nonadditive blood tube to be held for other ancillary testing.
The total protein via refractometer was 5.3 g/dL. The nucleated cell count derived from the in-clinic hematology analyzer (reported as WBCs) was 201 K/ul. Microscopically, the fluid was replete with degenerate neutrophils, fewer large mononuclear cells, and infrequent lymphocytes. Scattered cells contained intracellular bacterial cocci (Figure 2).
Alby’s results were consistent with an exudative effusion, i.e. a high protein fluid with markedly high cellularity and a predominance of neutrophils. The cytologic identification of bacteria confirmed the diagnosis of pyothorax.
These diagnostic results, taken together, allowed for prompt clinical management by the veterinary team in Alby’s case. This consisted of IV fluid therapy, drainage of the effusion after chest tube placement to allow suction and ongoing removal and actionable antimicrobial stewardship (initial antimicrobial therapy with marbofloxacin and ampicillin while pending culture), as per evidence- and expert-based guidelines.1
The rapid return of results enabled shared decision-making with Alby’s owners, together with communication of his prognosis and the need for ongoing monitoring.1 Culture and susceptibility testing from the non-additive tube identified Peptostreptococcus sp. and assisted with oral antibiotic choice moving forward.
Case 2) Willow’s chylothorax due to cardiomyopathy
Willow, a 16-year-old indoor-only domestic shorthair presented in respiratory distress after several days of hiding and inappetence. Radiographs identified pleural effusion, and therapeutic thoracocentesis was promptly performed.
The total protein on the fluid (Figure 3) obtained via refractometer was 5.0 g/dL. The nucleated cell count derived from the in-clinic hematology analyzer reported 1.72 K/ul.
To prepare a concentrated sample for cytologic evaluation, an aliquot of the fluid was centrifuged (similar to the preparation of urine sediment for microscopic review), and a drop of the concentrated fluid was transferred to a glass slide to make a smear. Microscopic review of the sediment smear identified mostly small lymphocytes and scattered erythrocytes in a proteinaceous background (Figure 4A). Higher magnification of the fluid revealed abundant, minute clear spaces throughout the concentrated proteinaceous background, most consistent with lipids (Figure 4B).
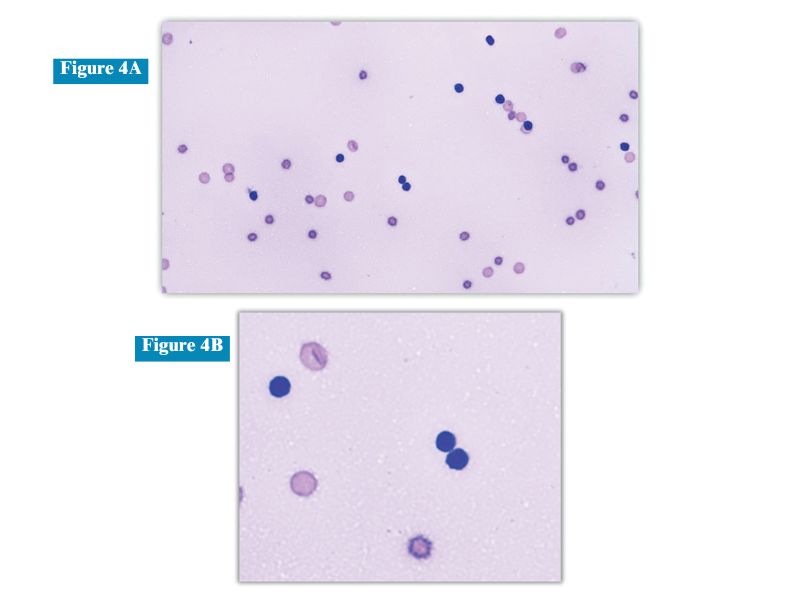
Willow’s effusion was categorized as a modified transudate due to its low cellularity with a disproportionately increased protein. The predominance of small lymphocytes and increased lipids in the background were most consistent with chylous origin. A fluid triglyceride level measured on a chemistry analyzer as greater than 100 mg/dl was utilized to confirm the suspected diagnosis of chylous effusion.2
Chylothorax in cats may be attributed to underlying heart disease. In Willow’s case, an abnormal NT-proBNP ELISA result prompted an echocardiogram that confirmed her underlying cardiomyopathy as the likely cause.3
Case 3) Bob’s feline infectious peritonitis (FIP)
Bob, a two-year-old indoor-only Maine Coon cat presented in respiratory distress. Radiographs identified pleural effusion and 40 ml of straw-colored fluid was removed via thoracocentesis.
The fluid total protein via refractometer was 8.0 g/dL, and the nucleated cell count derived from the in-clinic hematology analyzer reported 2.65 K/ul.
Microscopically, the fluid contained scattered vacuolated macrophages and fewer neutrophils (Figure 5A). Higher magnification revealed stippled pink protein in the background (Figure 5B).
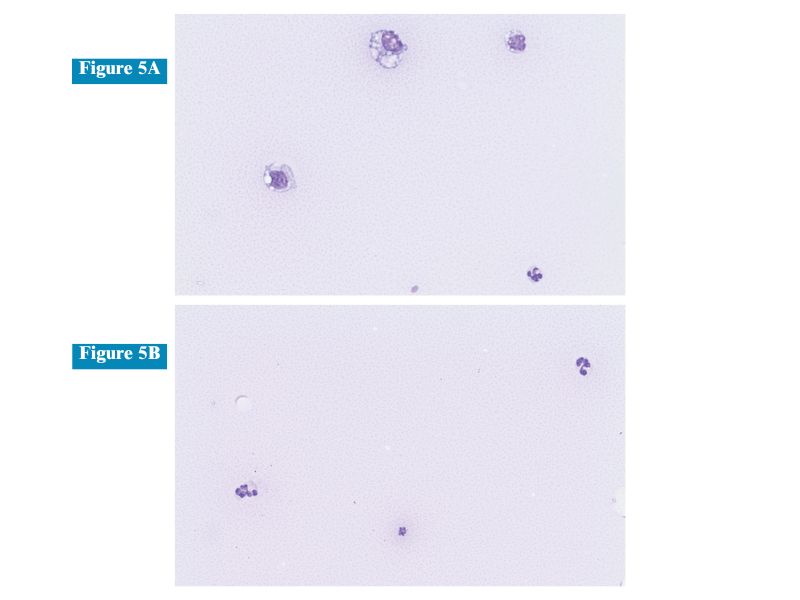
Bob’s findings were concerning for feline infectious peritonitis (FIP). While the nucleated cell count was only mildly elevated, the protein in the effusion was markedly elevated, and it was straw-colored and viscous. Protein measurements on the effusion via in-house chemistry analyzer reported a total protein of 8.9 g/dL and 1.9 g/dL albumin, with globulins calculated at
7.0 g/dL.
As per the FIP diagnosis consensus guidelines, an albumin:globulin ratio (A:G) >0.6 on an effusion essentially rules out underlying FIP,4 while an A:G <0.4 makes infection more likely.4,5
In Bob’s case, the fluid A:G ratio was 0.3 and, together with his signalment, clinical signs, and imaging findings, this supported the diagnosis of FIP.
Additional testing, such as PCR for the mutated coronavirus, was discussed with Bob’s owners to further support his suspected diagnosis, and prior to specific FIP therapy.5
Summary
In-clinic effusion analysis, combined with other in-house diagnostic testing at the point of care, can provide key diagnostic findings when needed quickly, as in many emergency cases. These test results are instrumental in assisting clinicians with planning the most appropriate course of treatment for dyspneic patients, as described here, and for communicating clinical management and prognosis to pet owners.
Helpful tools, such as using the in-clinic hematology analyzer to determine nucleated cell counts and total protein via refractometer or in-clinic chemistry analyzer, allow for better characterization of the effusions. These data are often coupled with cytologic analysis to confirm the cellular composition and observe unique background staining properties, which can aid diagnosis and target further testing.
Cats in respiratory distress require prompt, targeted management by veterinary teams to stabilize their critical status, determine cause, and rapidly define treatment needs. The option and utility of in-house diagnostic testing, and obtainment of imaging results (along with consultation with board-certified radiologists when needed), can reduce much of the stress and uncertainty of these cases for veterinary teams, and pet owners as well.
Holly Brown, DVM, PhD, DACVP, is a board-certified clinical pathologist with a passion for maximizing laboratory diagnostics for more informed and improved patient care. Dr. Brown currently serves as chief veterinary educator for Antech Diagnostics and enjoys educating veterinary teams on how to derive the most value from their labwork.
Michelle Evason, BSc, DVM, DACVIM (SAIM), MRCVS, serves as global director of Veterinary Clinical Education for Antech Diagnostics. Dr. Evason has worked in general practice, academia, specialty clinical practice, and in the animal health industry. She has published on numerous infectious diseases, antimicrobial stewardship, nutrition, spectrum of care, veterinary- and pet-owner education related topics.
References
- Lappin MR, Blondeau J, Boothe D, et al. Antimicrobial use Guidelines for Treatment of Respiratory Tract Disease in Dogs and Cats: Antimicrobial Guidelines Working Group of the International Society for Companion Animal Infectious Diseases. J Vet Intern Med. 2017;31(2):279-294.
- Waddle JR, Giger U. Lipoprotein electrophoresis differentiation of chylous and nonchylous pleural effusions in dogs and cats and its correlation with pleural effusion triglyceride concentration. Vet Clin Pathol.1990;19:80–85.
- Lu TL, Côté E, Kuo YW, Wu HH, Wang WY, Hung YW. Point-of-care N-terminal pro B-type natriuretic peptide assay to screen apparently healthy cats for cardiac disease in general practice. J Vet Intern Med. 2021;35(4):1663-1672.
- Jeffery U, Deitz K, Hostetter S. Positive predictive value of albumin: globulin ratio for feline infectious peritonitis in a mid-western referral hospital population. Journal of Feline Medicine and Surgery. 2012;14(12):903-905.
- Thayer V, Gogolski S, Felten S, Hartmann K, Kennedy M, Olah GA. 2022 AAFP/EveryCat Feline Infectious Peritonitis Diagnosis Guidelines. Journal of Feline Medicine and Surgery. 2022;24(9):905-933.