A salivary mucocele (sialocele) is an accumulation of saliva in the subcutaneous space due to damage to a salivary gland or duct. The leakage of saliva causes an inflammatory reaction under the skin and development of a fluid-filled “pocket.” There is no epithelial lining to this tissue, so these are not considered cysts.
Sialoceles are uncommon, accounting for about 0.3 percent of diagnostic submissions.1,2 They may occur due to trauma, neoplasia, or sialoliths, although idiopathic is the most common cause accounting for about 60 percent of salivary gland tissue submitted for histopathology.3 The affected gland(s) will determine the location of the saliva accumulation. Most sialoceles are nonpainful but can become large.
The treatment of choice for sialoceles is surgery. Surgical treatment offers a reliable, permanent solution for our patients. As with many conditions, successful outcome relies on accurate diagnosis, knowledge of relevant anatomy, and managing client expectations.
Relevant anatomy
Dogs and cats have four pairs of major salivary glands: mandibular, sublingual, zygomatic, and parotid. The parotid gland is located superficial to the vertical portion of the ear canal. The zygomatic gland is located ventral to the globe and medial to the zygomatic arch. A sialocele due to anomalies with this salivary gland will cause orbital swelling and exophthalmos. The mandibular salivary gland can be found just caudal to the angle of the mandible and is easily palpable. The sublingual salivary gland shares a capsule caudally with the mandibular salivary gland. As the gland travels rostrally it becomes less defined and forms clusters of salivary tissue.
Due to the close anatomic association of the mandibular and sublingual glands, they are considered a unit. A sialocele that forms from these two glands most commonly is in the cervical region. Less commonly, the sialocele is found in the pharynx and can cause difficulty breathing. Fluid accumulation under the tongue (ranula) is also seen with injury to this gland complex. The accumulation of saliva in the cervical region is generally nonpainful, but can become quite large. The remainder of this discussion will be focused on cervical sialoceles as they are by far the most commonly seen in practice.

Diagnosis
Fluctuant, nonpainful swelling in the upper cervical region is the most common presentation for salivary mucoceles in our canine patients. Some cases may present with unilateral swelling under the tongue (ranula) (Figure 1). Aspiration of the swelling typically produces a think, viscous fluid that is pink or yellow in color (Figure 2). Although some cases may improve temporarily with drainage, antibiotics, and anti-inflammatories, surgical excision of the affected glands is the definitive treatment.

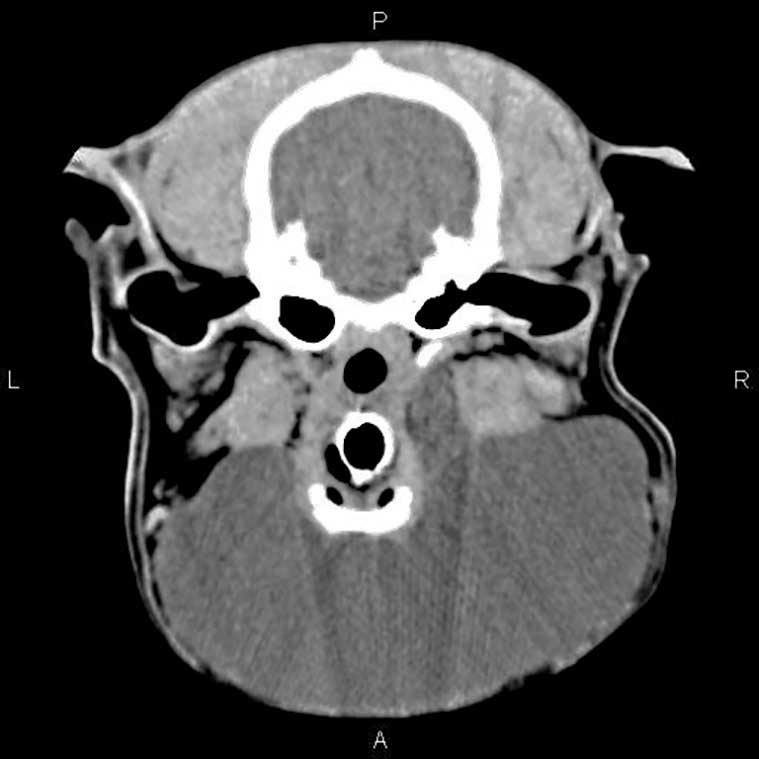
Cervical sialoceles can present as a ventral cervical swelling with no obvious lateralization. Prior to surgery, it is critical to determine which side is affected. Often, when the patient is placed in dorsal recumbency under general anesthesia, the sialocele will “fall” to the affected side. If it is still not obvious which side is involved, ultrasound or cross-sectional imaging can be pursued. (Figure 3). Ultrasound of a cervical sialocele identifies a round echogenic structure with anechoic fluid pocket. As the sialocele becomes more chronic, the fluid becomes less anechoic and more heterogenous.5
Surgery
Removal of the sublingual and mandibular salivary glands should be performed for treatment of cervical mucoceles. The patient can be positioned in either lateral recumbency with the affected side up or dorsal recumbency. A wide clip and prep are recommended to allow adequate exposure and exploration of the area. An incision is made caudal to the mandibular ramus over the palpable mandibular salivary gland and continued cranially toward the mandibular symphysis. The mandibular salivary gland is located just cranial to the jugular vein bifurcation. The platysma muscle is gently incised to expose this area. The mandibular lymph nodes are located just cranial and ventral to the bifurcation.
It is critical to differentiate the salivary gland (generally larger) from the lymph node so that the correct tissue is removed. Gentle dissection is continued until the capsule of the salivary gland is encountered. The capsule is incised, and the salivary gland dissected. The vasculature to the gland is located deeply (medial surface).
Once the vessels have been ligated, gentle traction is applied to the gland to allow dissection and continued exposure rostrally until the sublingual gland complex is removed (Figure 4).

This gland complex is located deep to the digastricus muscle. The duct is ligated as rostrally as possible, and the mandibular and sublingual gland complex removed as an entire unit. The lingual nerve is a good anatomic landmark for ligation of the duct.4 Most salivary mucoceles will resolve if the gland/duct complex is removed up to the lingual nerve. The mylohyoideus muscle is incised to identify this nerve. The area is lavaged and closed routinely.
If a ranula is present, marsupialization of the affected tissue can be completed. This is beneficial if the area is becoming traumatized by the patient. To complete this procedure, remove a full thickness section of tissue in an oval shape. Once this piece of tissue is removed, the mucosal edges are sutured to the lining of the sialocele. Small, absorbable monofilament suture is preferred. Marsupialization is not the definitive treatment for these patients as the mucosa will heal over time. Removal of the mandibular and sublingual glands is still required to prevent recurrence.
Post-operative care
The muscles and soft tissues are closed in routine fashion. Some surgeons will elect to drain the salivary mucocele and place a passive drain to facilitate rapid resolution of the sialocele.
Summary
Salivary mucoceles are uncommon in our veterinary patients. They can be seen after trauma (dental procedures, prong collars) but the cause is often unknown. Cervical mucoceles–nonpainful fluid accumulation originating from the mandibular and sublingual glands are the most common. Sometimes a ranula is also present. Surgery offers a definitive treatment with an excellent prognosis.
Knowledge of anatomy is critical to provide an ideal outcome. Recurrence of the mucocele is usually due to incomplete removal of the mandibular/sublingual salivary gland complex. Some patients will develop the same condition on the opposite side in the future.6
Kendra Freeman DVM, MS, DACVS, is a graduate of Colorado State University and maintains dual certification with the American College of Veterinary Surgeons. Dr. Freeman is an associate surgeon in Albuquerque, N.M. Her case load consists of orthopedics, general soft tissue, and sports medicine cases with the occasional return to her roots in large animal lameness and surgery.
References
- Waldron DR, Smith MM. Salivary mucoceles. Probl Vet Med. 1991 Jun;3(2):270-6. PMID: 1802253.
- Spangler WL, Culbertson MR. Salivary gland disease in dogs and cats: 245 cases (1985-1988). J Am Vet Med Assoc. 1991 Feb 1;198(3):465-9. PMID: 2010345.
- Lieske DE, Rissi DR. A retrospective study of salivary gland diseases in 179 dogs (2010–2018). Journal of Veterinary Diagnostic Investigation. 2020;32(4):604-610.
- Tobias, Karen M., and Spencer A. Johnston. Veterinary surgery: small animal. Elsevier Health Sciences, 2013.
- Torad, F.A. and Hassan, E.A. (2013), CLINICAL AND ULTRASONOGRAPHIC CHARACTERISTICS OF SALIVARY MUCOCELES IN 13 DOGS. Veterinary Radiology & Ultrasound, 54: 293-298.
- Poirier VJ, Mayer-Stankeová S, Buchholz J, Vail DM, Kaser Hotz B. Efficacy of Radiation Therapy for the Treatment of Sialocele in Dogs. J Vet Intern Med. 2018 Jan;32(1):107-110. doi: 10.1111/jvim.14868. Epub 2017 Nov 13.